

Performance of intensive care unit severity scoring systems across different ethnicities in the USA: a retrospective observational study
- PMID: 33766288
- PMCID: PMC8063502
- DOI: 10.1016/S2589-7500(21)00022-4
Performance of intensive care unit severity scoring systems across different ethnicities in the USA: a retrospective observational study
Abstract
Background: Despite wide use of severity scoring systems for case-mix determination and benchmarking in the intensive care unit (ICU), the possibility of scoring bias across ethnicities has not been examined. Guidelines on the use of illness severity scores to inform triage decisions for allocation of scarce resources, such as mechanical ventilation, during the current COVID-19 pandemic warrant examination for possible bias in these models. We investigated the performance of the severity scoring systems Acute Physiology and Chronic Health Evaluation IVa (APACHE IVa), Oxford Acute Severity of Illness Score (OASIS), and Sequential Organ Failure Assessment (SOFA) across four ethnicities in two large ICU databases to identify possible ethnicity-based bias.
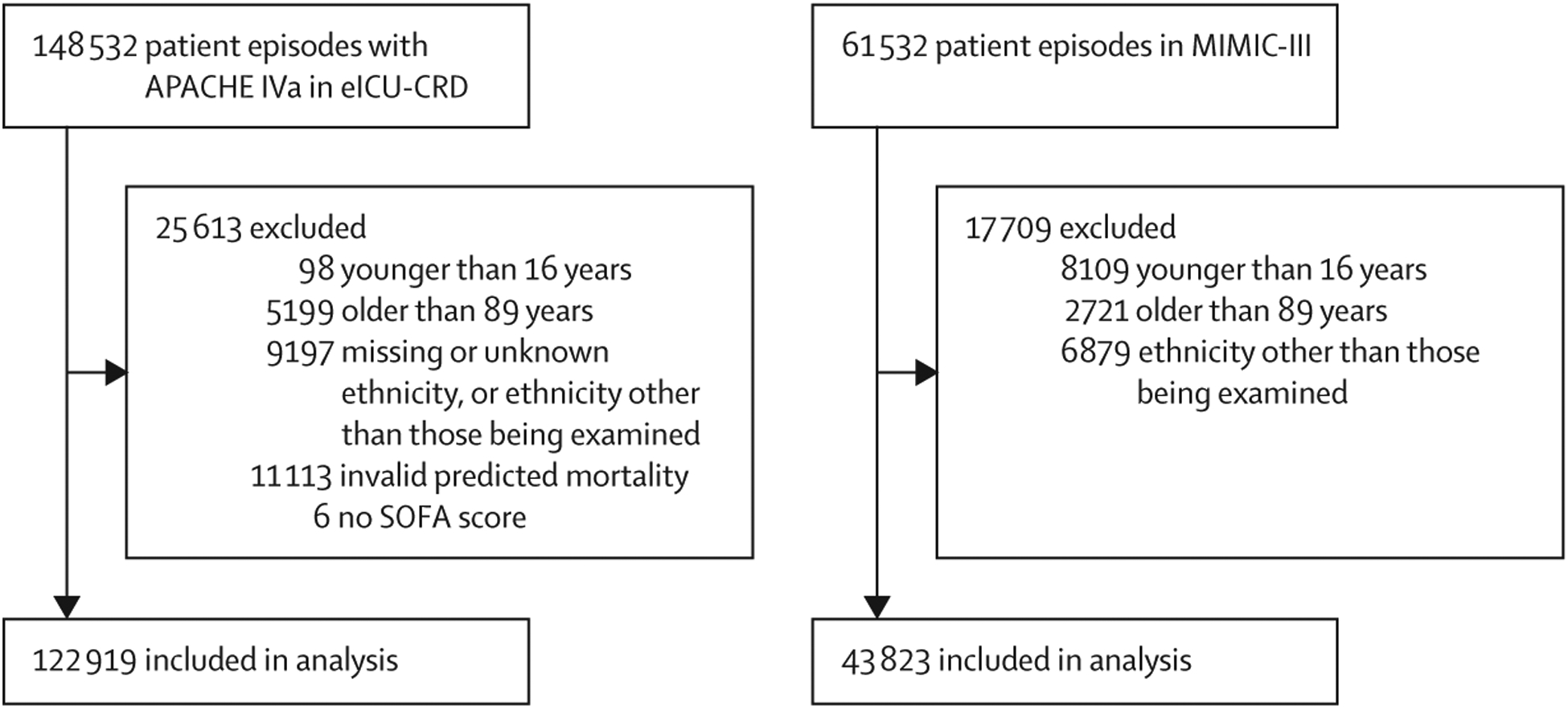
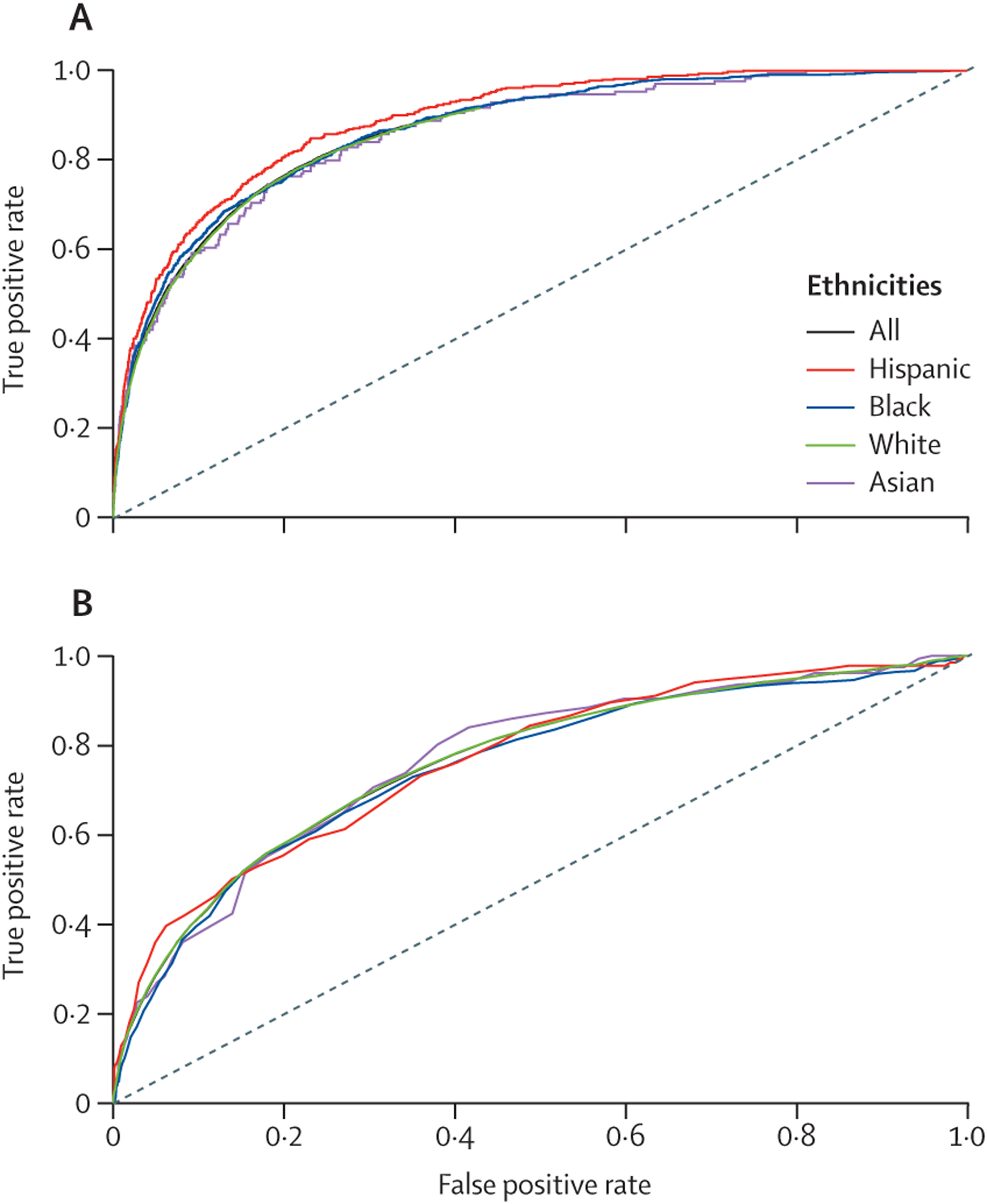
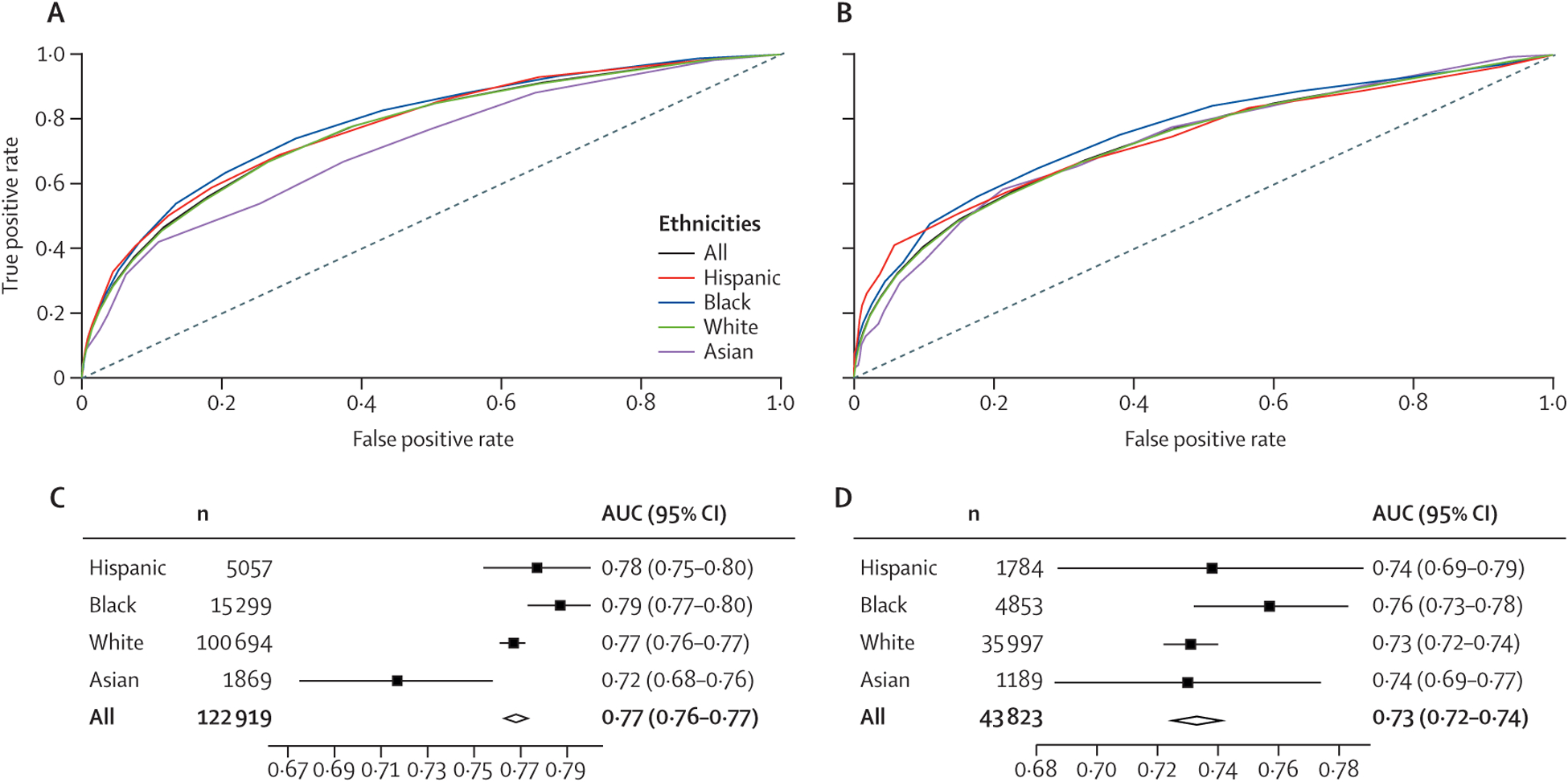
Methods: Data from the electronic ICU Collaborative Research Database (eICU-CRD) and the Medical Information Mart for Intensive Care III (MIMIC-III) database, built from patient episodes in the USA from 2014-15 and 2001-12, respectively, were analysed for score performance in Asian, Black, Hispanic, and White people after appropriate exclusions. Hospital mortality was the outcome of interest. Discrimination and calibration were determined for all three scoring systems in all four groups, using area under receiver operating characteristic (AUROC) curve for different ethnicities to assess discrimination, and standardised mortality ratio (SMR) or proxy measures to assess calibration.
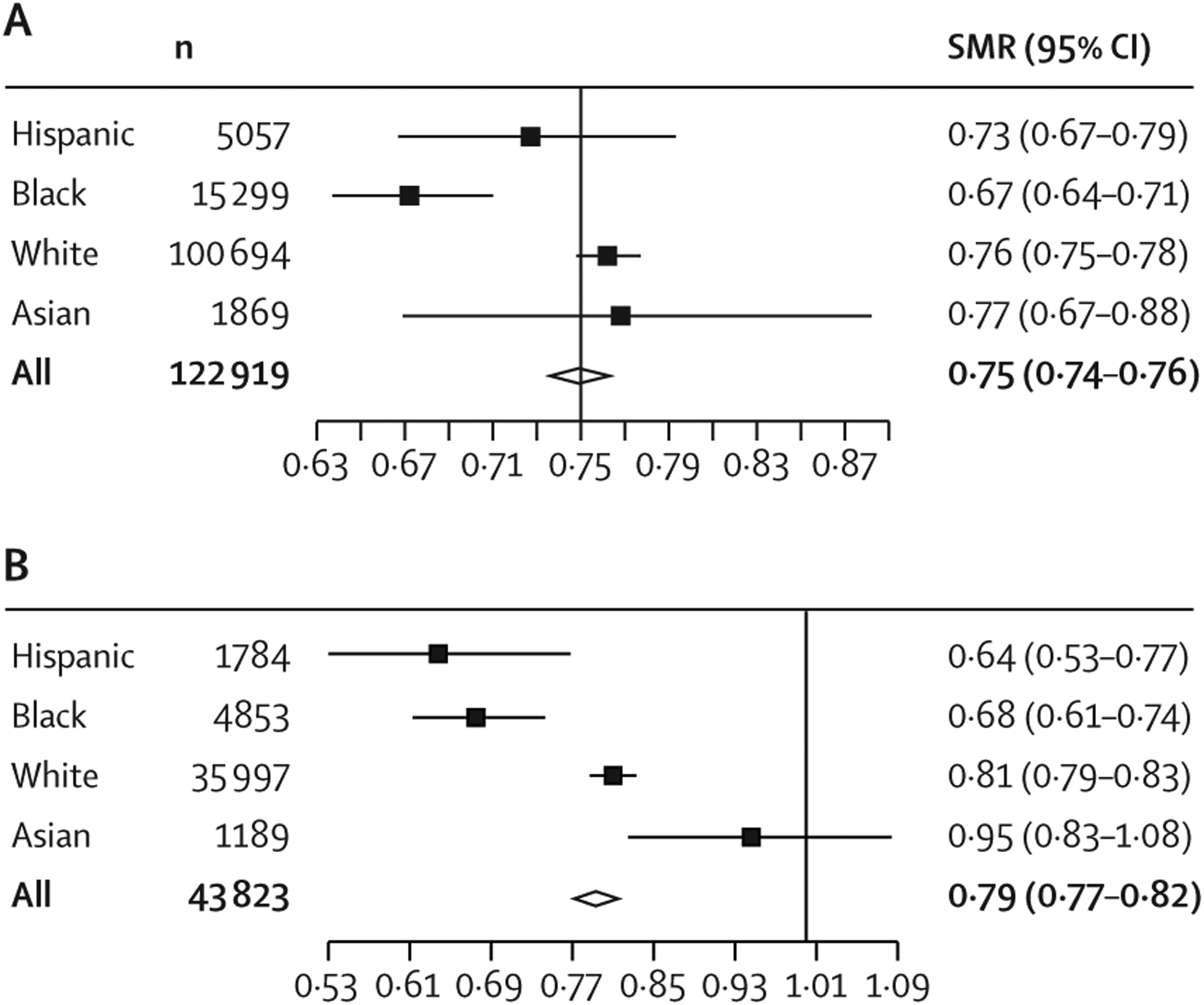
Findings: We analysed 166 751 participants (122 919 eICU-CRD and 43 832 MIMIC-III). Although measurements of discrimination were significantly different among the groups (AUROC ranging from 0·86 to 0·89 [p=0·016] with APACHE IVa and from 0·75 to 0·77 [p=0·85] with OASIS), they did not display any discernible systematic patterns of bias. However, measurements of calibration indicated persistent, and in some cases statistically significant, patterns of difference between Hispanic people (SMR 0·73 with APACHE IVa and 0·64 with OASIS) and Black people (0·67 and 0·68) versus Asian people (0·77 and 0·95) and White people (0·76 and 0·81). Although calibrations were imperfect for all groups, the scores consistently showed a pattern of overpredicting mortality for Black people and Hispanic people. Similar results were seen using SOFA scores across the two databases.
Interpretation: The systematic differences in calibration across ethnicities suggest that illness severity scores reflect statistical bias in their predictions of mortality.
Funding: There was no specific funding for this study.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests
RS received writing fees for health-care reports from Crystallise UK.
CM is a director for Crystallise UK. HM, JWG, DJS, and LAC declare no competing interests.
Figures
Update of
-
Performance of intensive care unit severity scoring systems across different ethnicities.medRxiv [Preprint]. 2021 Jan 20:2021.01.19.21249222. doi: 10.1101/2021.01.19.21249222. medRxiv. 2021. Update in: Lancet Digit Health. 2021 Apr;3(4):e241-e249. doi: 10.1016/S2589-7500(21)00022-4. PMID: 33501459 Free PMC article. Updated. Preprint.
Comment in
-
Ethnicity-based bias in clinical severity scores.Lancet Digit Health. 2021 Apr;3(4):e209-e210. doi: 10.1016/S2589-7500(21)00044-3. Lancet Digit Health. 2021. PMID: 33766286 No abstract available.
References
-
- Wiens J, Price WN 2nd, Sjoding MW. Diagnosing bias in data-driven algorithms for healthcare. Nat Med 2020; 26: 25–26. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
