

Brachial plexopathy as a complication of COVID-19
- PMID: 33766961
- PMCID: PMC8006770
- DOI: 10.1136/bcr-2020-237459
Brachial plexopathy as a complication of COVID-19
Abstract
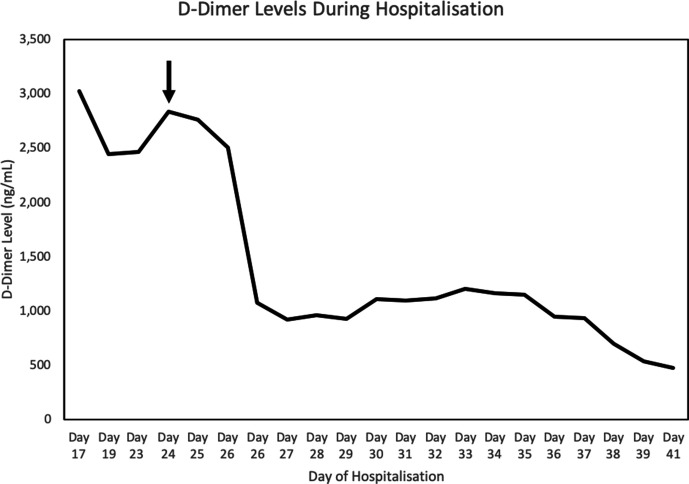
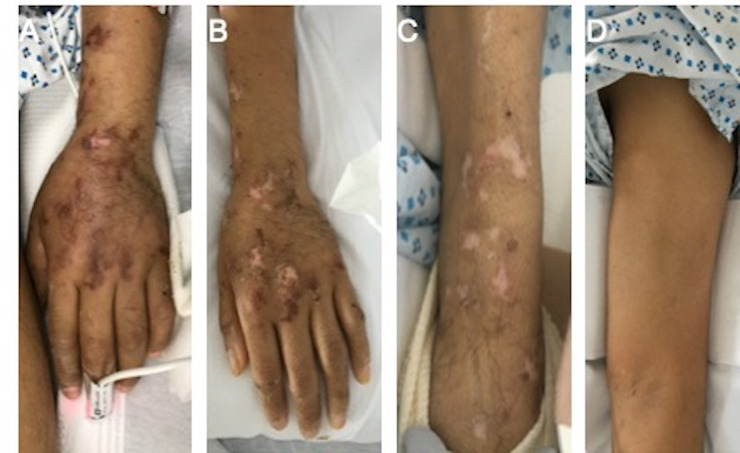
COVID-19 affects a wide spectrum of organ systems. We report a 52-year-old man with hypertension and newly diagnosed diabetes mellitus who presented with hypoxic respiratory failure due to COVID-19 and developed severe brachial plexopathy. He was not treated with prone positioning respiratory therapy. Associated with the flaccid, painfully numb left upper extremity was a livedoid, purpuric rash on his left hand and forearm consistent with COVID-19-induced microangiopathy. Neuroimaging and electrophysiological data were consistent with near diffuse left brachial plexitis with selective sparing of axillary, suprascapular and pectoral fascicles. Given his microangiopathic rash, elevated D-dimers and paucifascicular plexopathy, we postulate a patchy microvascular thrombotic plexopathy. Providers should be aware of this significant and potentially under-recognised neurologic complication of COVID-19.
Keywords: infections; neurological injury; neuromuscular disease; pain (neurology); peripheral nerve disease.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
-
- Weekly epidemiological update – 24 November 2020. World Health Organization 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical