

Does diagnostic uncertainty increase antibiotic prescribing in primary care?
- PMID: 33767206
- PMCID: PMC7994848
- DOI: 10.1038/s41533-021-00229-9
Does diagnostic uncertainty increase antibiotic prescribing in primary care?
Abstract
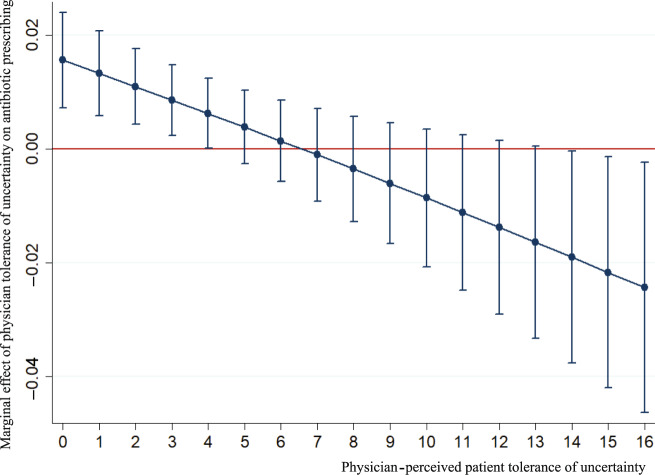
This study aimed to determine the association between factors relevant to diagnostic uncertainty and physicians' antibiotic-prescribing behaviour in primary care. A questionnaire survey was conducted on 327 physicians that measured their diagnostic ability, perceived frequency of diagnostic uncertainty, tolerance, and perceived patient tolerance of uncertainty. Physician antibiotic-prescribing behaviours were assessed based on their prescriptions (n = 207,804) of three conditions: upper respiratory tract infections (URTIs, antibiotics not recommended), acute tonsillitis (cautious use of antibiotics), and pneumonia (antibiotics recommended). A two-level logistic regression model determined the association between diagnostic uncertainty factors and physician antibiotic prescribing. Physicians perceived a higher frequency of diagnostic uncertainty resulting in higher antibiotic use for URTIs and less antibiotic use for pneumonia. Higher antibiotic use for acute tonsillitis was related to a low tolerance of uncertainty of physicians and patients. This study suggests that reducing diagnostic uncertainty and improving physician and patient uncertainty management could reduce antibiotic use.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
