

School-based screening and treatment may reduce P. falciparum transmission
- PMID: 33767384
- PMCID: PMC7994823
- DOI: 10.1038/s41598-021-86450-5
School-based screening and treatment may reduce P. falciparum transmission
Abstract
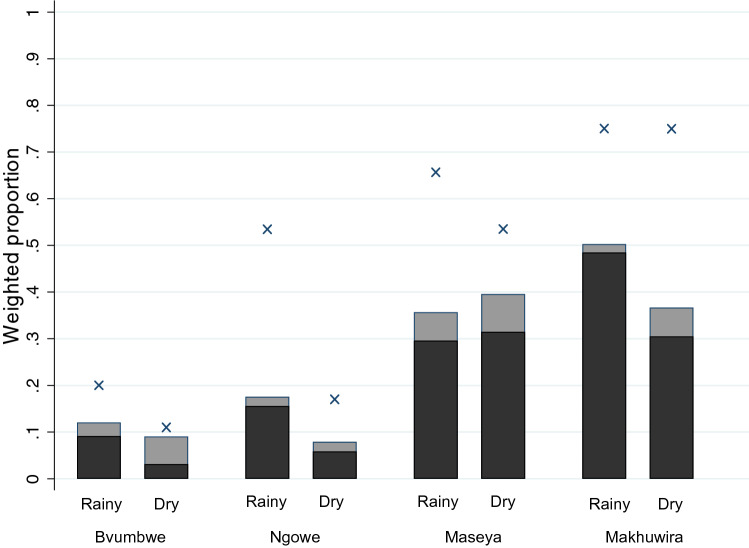
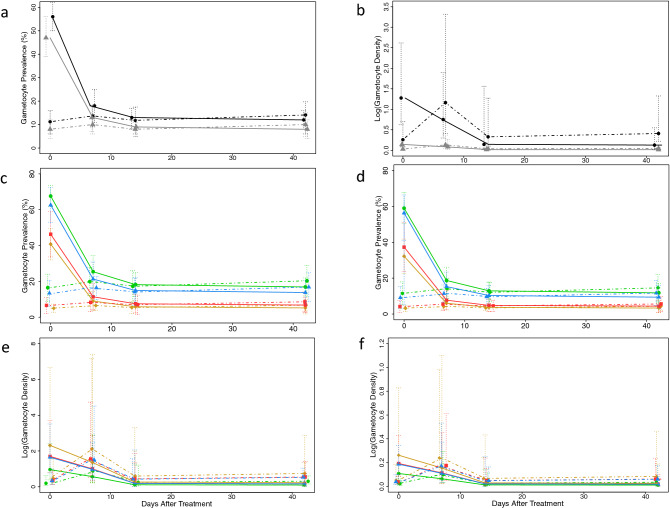
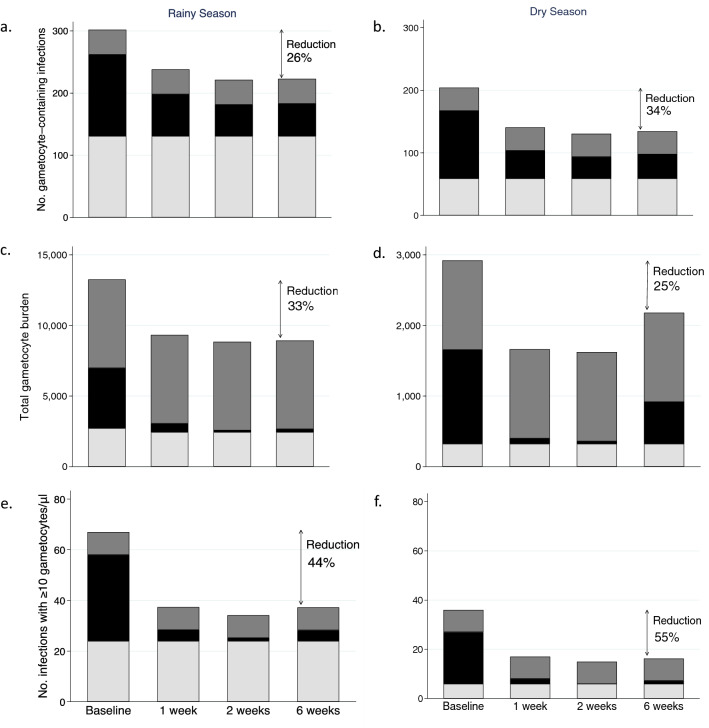
In areas where malaria remains entrenched, novel transmission-reducing interventions are essential for malaria elimination. We report the impact screening-and-treatment of asymptomatic Malawian schoolchildren (n = 364 in the rainy season and 341 in the dry season) had on gametocyte-the parasite stage responsible for human-to-mosquito transmission-carriage. We used concomitant household-based surveys to predict the potential reduction in transmission in the surrounding community. Among 253 students with P. falciparum infections at screening, 179 (71%) had infections containing gametocytes detected by Pfs25 qRT-PCR. 84% of gametocyte-containing infections were detected by malaria rapid diagnostic test. While the gametocyte prevalence remained constant in untreated children, treatment with artemether-lumefantrine reduced the gametocyte prevalence (p < 0.0001) from 51.8 to 9.7% and geometric mean gametocyte density (p = 0.008) from 0.52 to 0.05 gametocytes/microliter. In community surveys, 46% of all gametocyte-containing infections were in school-age children, who comprised only 35% of the population. Based on these estimates six weeks after the intervention, the gametocyte burden in the community could be reduced by 25-55% depending on the season and the measure used to characterize gametocyte carriage. Thus, school-based interventions to treat asymptomatic infections may be a high-yield approach to not only improve the health of schoolchildren, but also decrease malaria transmission.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- World Health Organization. World Malaria Report 2019. Geneva. (2019). Licence: CC BY-NC-SA 3.0 IGO
-
- WHO. Global technical strategy for malaria 2016–2030. World Health Organization (2015).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
