

Olfactory Dysfunction in Frontline Health Care Professionals During COVID-19 Pandemic in Brazil
- PMID: 33767631
- PMCID: PMC7985267
- DOI: 10.3389/fphys.2021.622987
Olfactory Dysfunction in Frontline Health Care Professionals During COVID-19 Pandemic in Brazil
Abstract
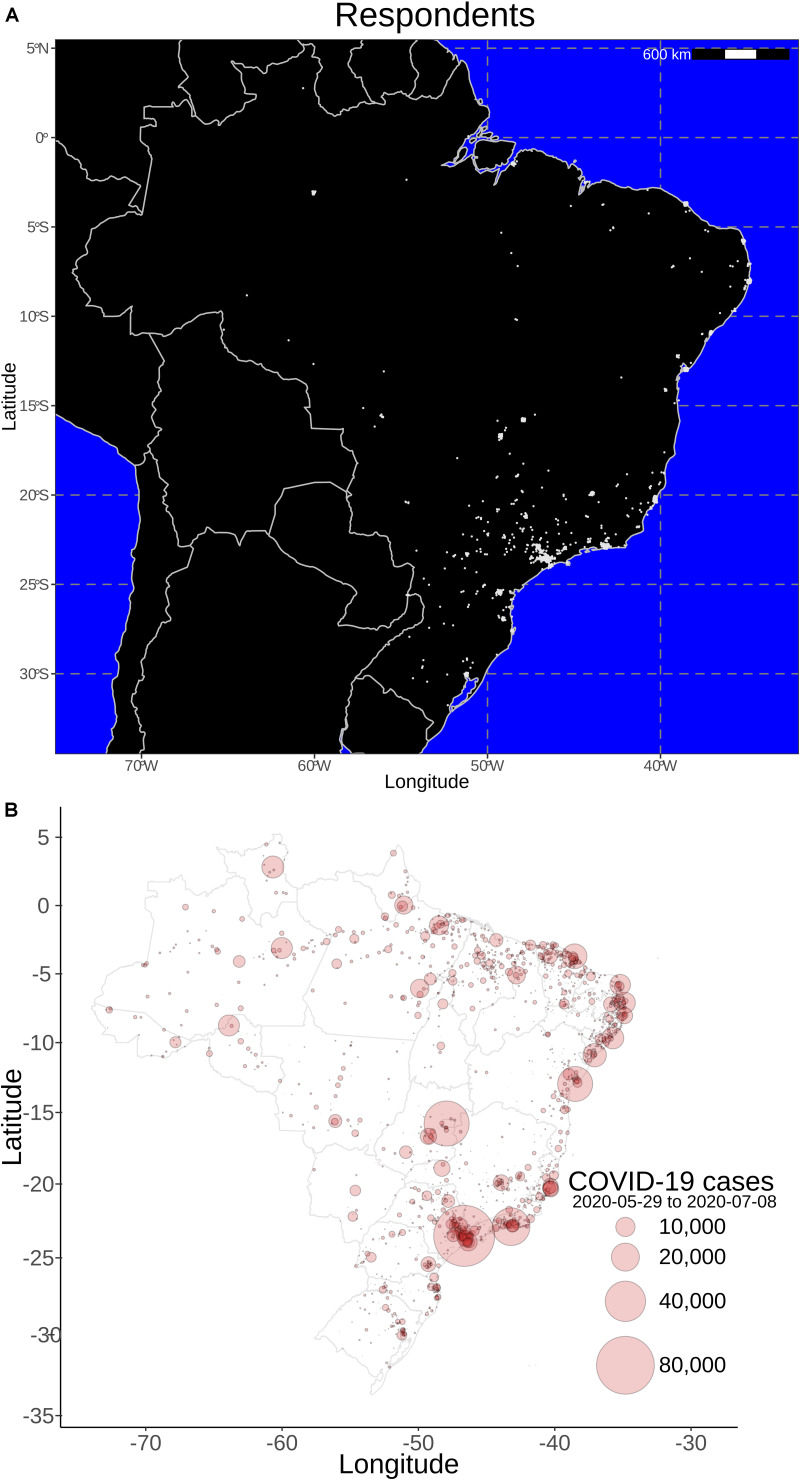
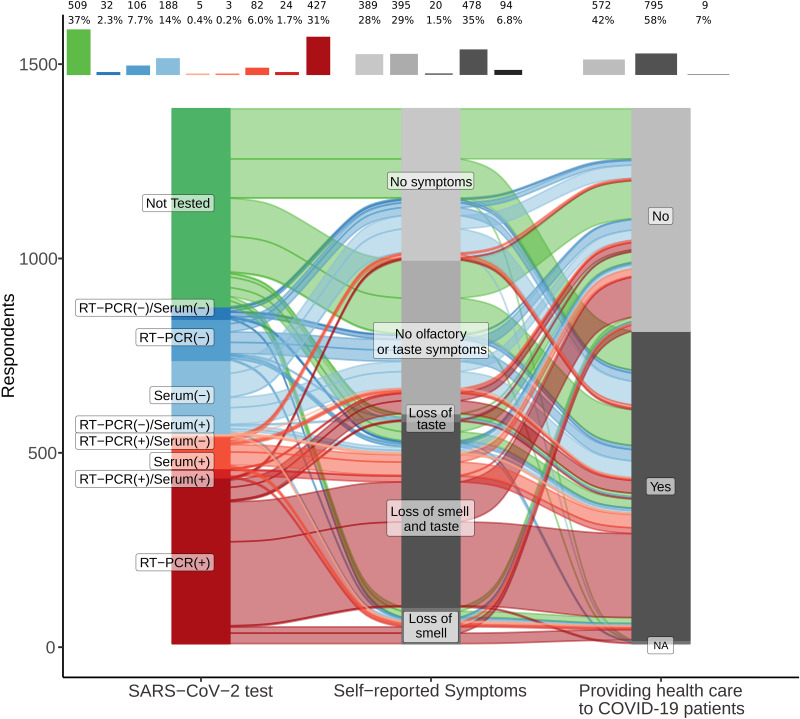
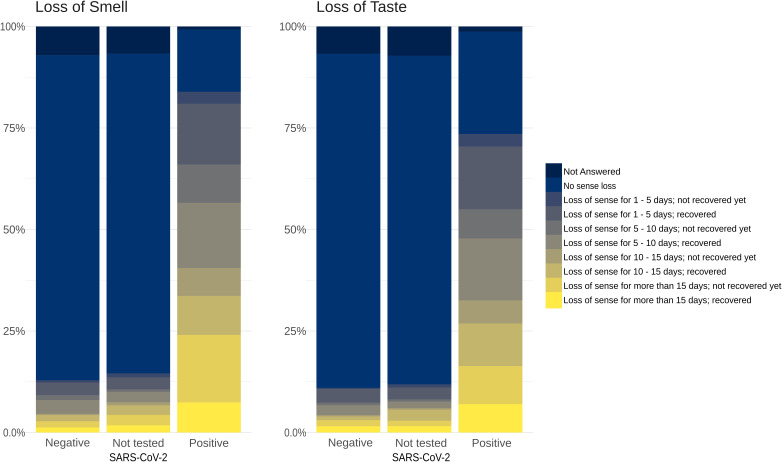
Upper respiratory viral infections can decrease the sense of smell either by inflammatory restriction of nasal airflow that carries the odorant molecules or through interference in olfactory sensory neuron function. During the coronavirus disease 2019 (COVID-19) pandemic, triggered by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), worldwide reports of severe smell loss (anosmia/hyposmia) revealed a different type of olfactory dysfunction associated with respiratory virus infection. Since self-reported perception of smell is subjective and SARS-CoV-2 exposure is variable in the general population, we aimed to study a population that would be more homogeneously exposed to the virus. Here, we investigated the prevalence of olfactory loss in frontline health professionals diagnosed with COVID-19 in Brazil, one of the major epicenters of the disease. We also analyzed the rate of olfactory function recovery and the particular characteristics of olfactory deficit in this population. A widely disclosed cross-sectional online survey directed to health care workers was developed by a group of researchers to collect data concerning demographic information, general symptoms, otolaryngological symptoms, comorbidities, and COVID-19 test results. Of the 1,376 health professionals who completed the questionnaire, 795 (57.8%) were working directly with COVID-19 patients, either in intensive care units, emergency rooms, wards, outpatient clinics, or other areas. Five-hundred forty-one (39.3%) participants tested positive for SARS-CoV-2, and 509 (37%) were not tested. Prevalence of olfactory dysfunction in COVID-19-positive subjects was 83.9% (454 of 541) compared to 12.9% (42 of 326) of those who tested negative and to 14.9% (76 of 509) of those not tested. Olfactory dysfunction incidence was higher in those working in wards, emergency rooms, and intensive care units compared to professionals in outpatient clinics. In general, remission from olfactory symptoms was frequent by the time of responses. Taste disturbances were present in 74.1% of infected participants and were significantly associated with hyposmia. In conclusion, olfactory dysfunction is highly correlated with exposure to SARS-CoV-2 in health care professionals, and remission rates up to 2 weeks are high.
Keywords: COVID-19; SARS-CoV-2; anosmia; coronavirus; health care; olfaction disorders; respiratory tract infection; sense of smell.
Copyright © 2021 Sbrana, Fornazieri, Bruni-Cardoso, Avelino-Silva, Schechtman, Voegels, Malnic, Glezer and de Rezende Pinna.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Baig A. M., Khaleeq A., Ali U., Syeda H. (2020). Evidence of COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and proposed neurotropic mechanism. ACS Chem. Neurosci. 11 995–998. - PubMed
-
- Beltran-Corbelini A., Chico-Garcia J. L., Martinez-Poles J., Rodriguez-Jorge F., Natera-Villalba E., Gomez-Corral J., et al. (2020). Acute-onset smell and taste disorders in the context of COVID-19: a pilot multicenter polymerase chain reaction based case-control study. Eur. J. Neurol. 27 1738–1741. 10.1111/ene.14273 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous