

Tumors and pseudotumors of the soft tissues: Imaging semiology and strategy
- PMID: 33767905
- PMCID: PMC7981940
- DOI: 10.25259/JCIS_135_2020
Tumors and pseudotumors of the soft tissues: Imaging semiology and strategy
Abstract
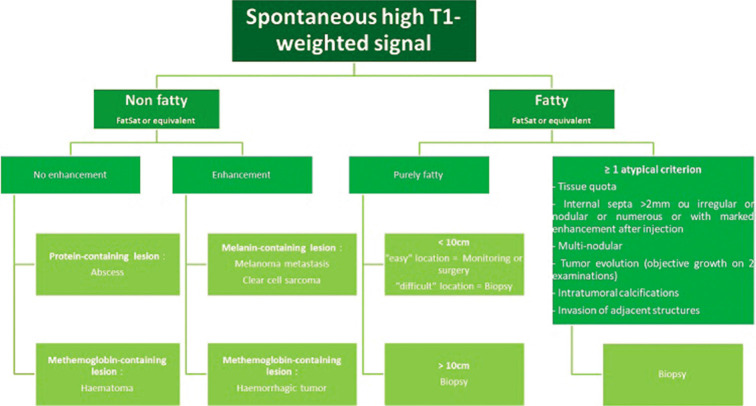
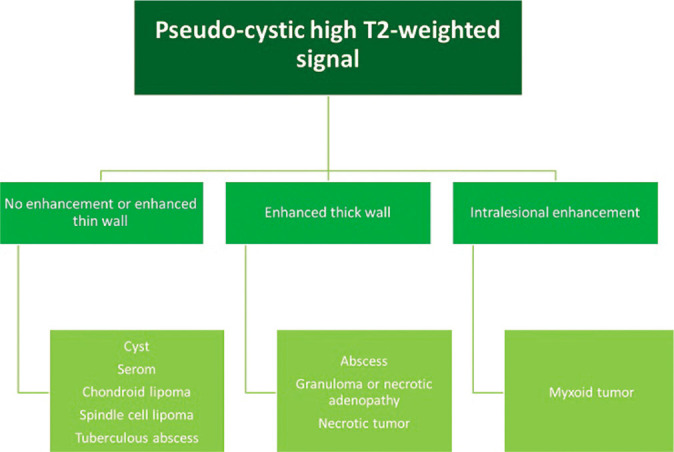
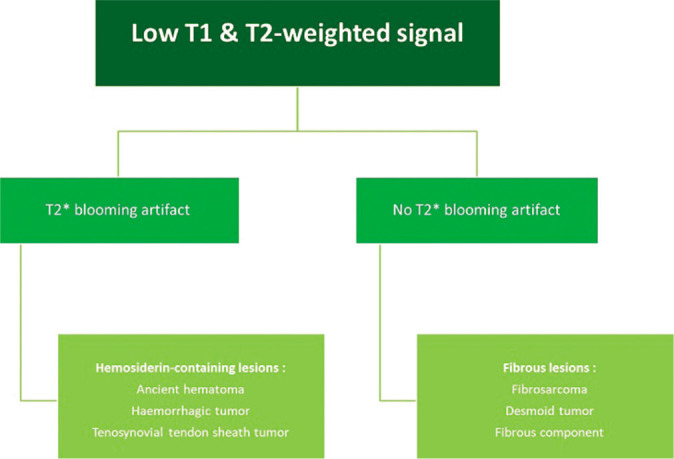
The aims of this educational review are to learn the semiological basis of soft-tissue lesions and, with the help of diagnostic algorithms, to apply the current recommendations for the management of soft-tissue tumors. Pseudotumors must first be identified and excluded. Among primary tumors, the search for macroscopic fat content on MRI is decisive; since it restricts the diagnostic range to adipocytic tumors. Key imaging features of non-adipocytic tumors are highlighted. When a deep soft-tissue mass is found, therapeutic abstention or simple monitoring is only appropriate when there is diagnostic certainty: This is only the case for typical pseudotumors, typical benign tumors, and fat tumors without atypical criteria. In all other cases, histological evidence is required. If there is any suspicion of soft-tissue sarcoma or any undetermined lesion, the patient should be referred to a sarcoma referral center before biopsy.
Keywords: Adipocytic tumor; Lipoma; Liposarcoma; Non-adipocytic tumor; Soft-tissue sarcoma.
© 2020 Published by Scientific Scholar on behalf of Journal of Clinical Imaging Science.
Conflict of interest statement
There are no conflicts of interest.
Figures
References
-
- Laredo JD, Wybier M, Petrover D. Netherlands: Elsevier; 2016. Imagerie Rhumatologique et Orthopédique.
-
- Cotten A. Netherlands: Elsevier, Masson; 2013. Pseudo-Tumeurs des Tissus Mous, in Imagerie Musculosquelettique: Pathologies Générales.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources