

Hepatic Steatosis Predicts Higher Incidence of Recurrence in Colorectal Cancer Liver Metastasis Patients
- PMID: 33767997
- PMCID: PMC7986714
- DOI: 10.3389/fonc.2021.631943
Hepatic Steatosis Predicts Higher Incidence of Recurrence in Colorectal Cancer Liver Metastasis Patients
Erratum in
-
Corrigendum: Hepatic Steatosis Predicts Higher Incidence of Recurrence in Colorectal Cancer Liver Metastasis Patients.Front Oncol. 2021 Aug 18;11:742987. doi: 10.3389/fonc.2021.742987. eCollection 2021. Front Oncol. 2021. PMID: 34490128 Free PMC article.
Abstract
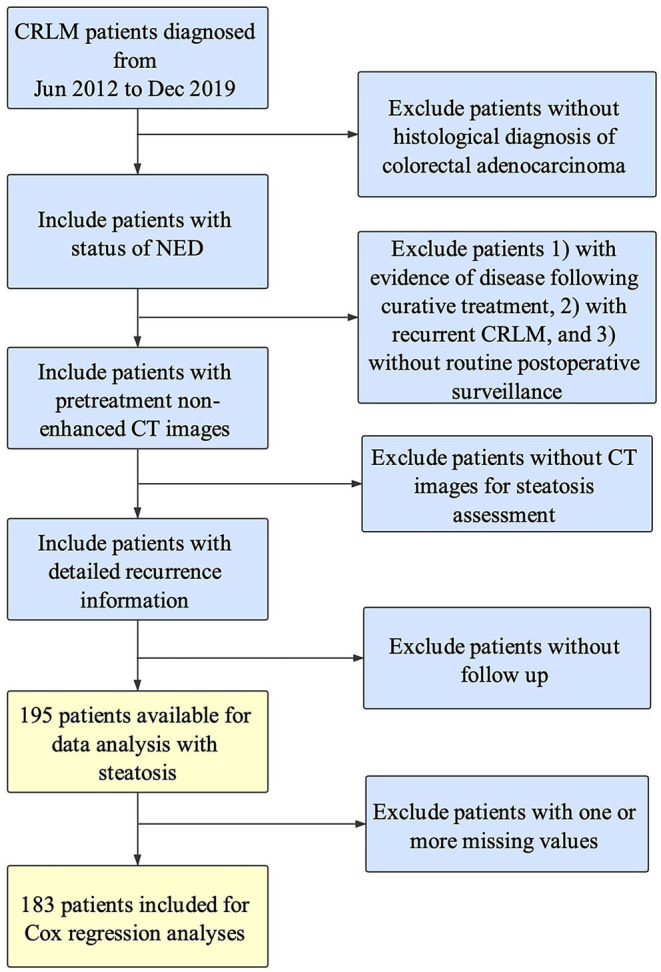
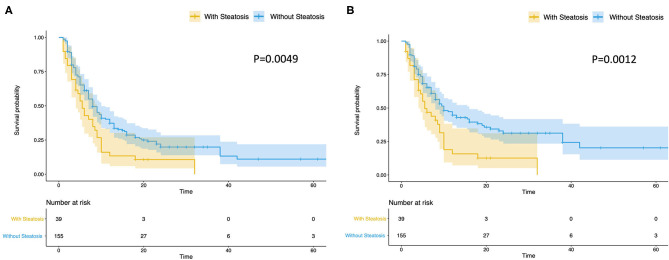
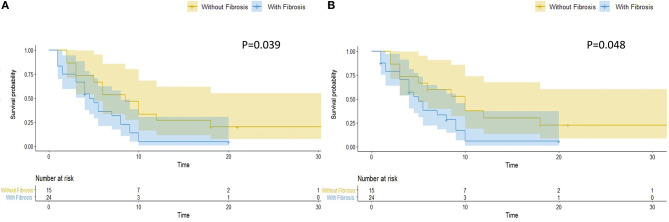
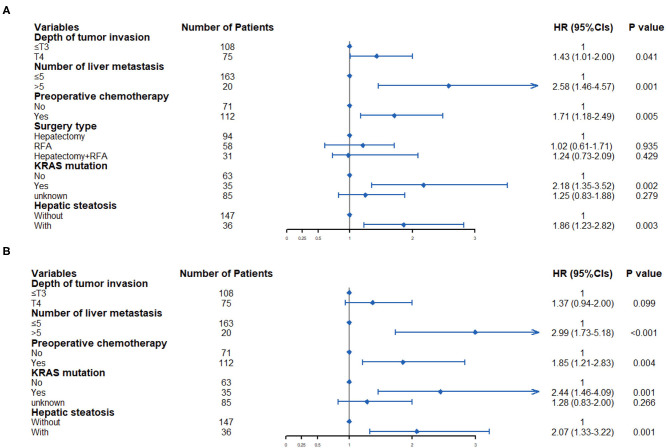
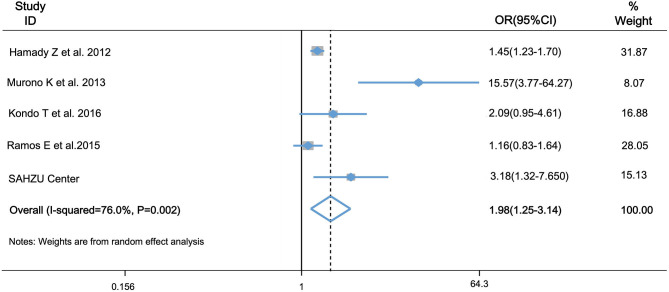
Purpose: Colorectal liver metastasis (CRLM) is the major cause of death due to colorectal cancer. Although great efforts have been made in treatment of CRLM, about 60-70% of patients will develop hepatic recurrence. Hepatic steatosis was reported to provide fertile soil for metastasis. However, whether hepatic steatosis predicts higher incidence of CRLM recurrence is not clear. Therefore, we aimed to determine the role of hepatic steatosis in CRLM recurrence in the present study. Methods: Consecutive CRLM patients undergoing curative treatment were retrospectively enrolled and CT liver-spleen attenuation ratio was used to detect the presence of hepatic steatosis. In patients with hepatic steatosis, we also detected the presence of fibrosis. Besides, a systematic literature search was performed to do meta-analysis to further analyze the association between hepatic steatosis and CRLM recurrence. Results: A total of 195 eligible patients were included in our center. Patients with hepatic steatosis had a significantly worse overall (P = 0.0049) and hepatic recurrence-free survival (RFS) (P = 0.0012). Univariate and multivariate analysis confirmed its essential role in prediction of RFS. Besides, hepatic fibrosis is associated with worse overall RFS (P = 0.039) and hepatic RFS (P = 0.048). In meta-analysis, we included other four studies, with a total of 1,370 patients in the case group, and 3,735 patients in the control group. The odds ratio was 1.98 (95% CI: 1.25-3.14, P = 0.004), indicating that patients with steatosis had a significantly higher incidence of CRLM recurrence. Conclusion: In summary, patients with hepatic steatosis had a significantly worse overall and hepatic RFS and it's associated with higher incidence of CRLM recurrence.
Keywords: L/S ratio; colorectal cancer; hepatic recurrence; hepatic steatosis; liver metastasis.
Copyright © 2021 Chen, Dai, Fang, Chen, Jiang, Wei and Ding.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources