

Cardiomyopathy in the peripartum period due to left ventricular non-compaction and association with Ebstein's anomaly: a case report
- PMID: 33768196
- PMCID: PMC7983311
- DOI: 10.1093/ehjcr/ytab088
Cardiomyopathy in the peripartum period due to left ventricular non-compaction and association with Ebstein's anomaly: a case report
Abstract
Background: Left ventricular non-compaction (LVNC) cardiomyopathy is a persistence of abnormal foetal myocardium and is a rare cause of cardiomyopathy in the peripartum period. Unlike other causes of peripartum cardiomyopathy which typically improve, LVNC has significant long-term personal and family implications and needs lifelong follow-up.
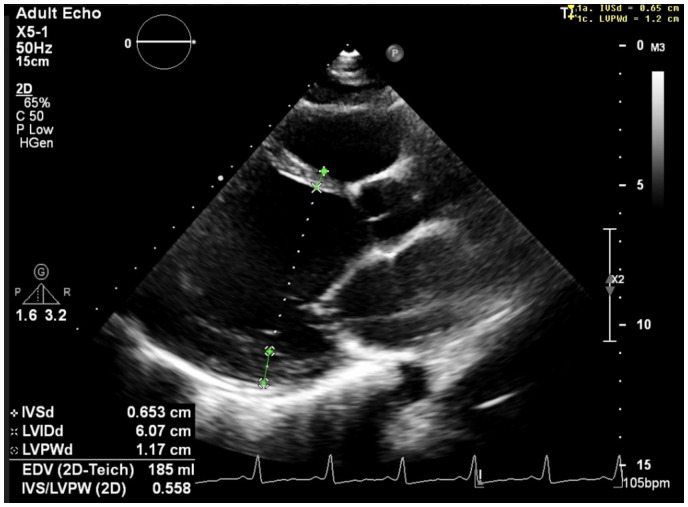
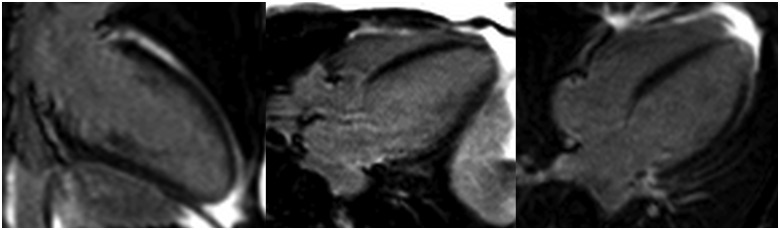
Case summary: We describe a unique case of a 30-year-old woman who developed cardiomyopathy in the peripartum period which was revealed on cardiovascular magnetic resonance imaging to be due to occult LVNC. Our patient also had Ebstein's anomaly, which is a known LVNC association.
Discussion: Cardiomyopathy in the peripartum period can be a decompensation of previously asymptomatic subclinical cardiomyopathy. It is important to assess for LVNC in patients presenting with this. Cardiovascular magnetic resonance imaging is the gold-standard imaging modality and allows accurate diagnosis of LVNC, associated structural complications and rare associations such as Ebstein's anomaly. Left ventricular non-compaction is irreversible and has implications for patients and their family members.
Keywords: Cardiovascular magnetic resonance; Case report; Ebstein’s anomaly; Echocardiography; Left ventricular non-compaction; Peripartum cardiomyopathy.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures





References
-
- Elliott P, Andersson B, Arbustini E, Bilinska Z, Cecchi F, Charron P. et al. Classification of the cardiomyopathies: a position statement from the European Society of Cardiology Working Group on myocardial and pericardial diseases. Eur Heart J 2007;29:270–276. - PubMed
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnet D, Council on Epidemiology and Prevention et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation 2006;113:1807–1816. - PubMed
-
- Hussein A, Karimianpour A, Collier P, Krasuski RA.. Isolated noncompaction of the left ventricle in adults. J Am Coll Cardiol 2015;66:578–585. - PubMed
-
- Regitz-Zagrosek V, Roos-Hesselink J, Blomstrom-Lundqvist C, Cifkova R, Dr Bonis M, Lung B. et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy: the Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur Heart J 2011;32:3147–3197. - PubMed
-
- Petersen SE, Selvanayagam JB, Wiesmann F, Robson MD, Francis JM, Anderson RH. et al. Left ventricular non-compaction: insights from cardiovascular magnetic resonance imaging. J Am Coll Cardiol 2005;46:101–105. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources