

Incidence and outcomes of perioperative myocardial infarction/injury diagnosed by high-sensitivity cardiac troponin I
- PMID: 33768367
- PMCID: PMC8405484
- DOI: 10.1007/s00392-021-01827-w
Incidence and outcomes of perioperative myocardial infarction/injury diagnosed by high-sensitivity cardiac troponin I
Abstract
Background: Perioperative myocardial infarction/injury (PMI) diagnosed by high-sensitivity troponin (hs-cTn) T is frequent and a prognostically important complication of non-cardiac surgery. We aimed to evaluate the incidence and outcome of PMI diagnosed using hs-cTnI, and compare it to PMI diagnosed using hs-cTnT.
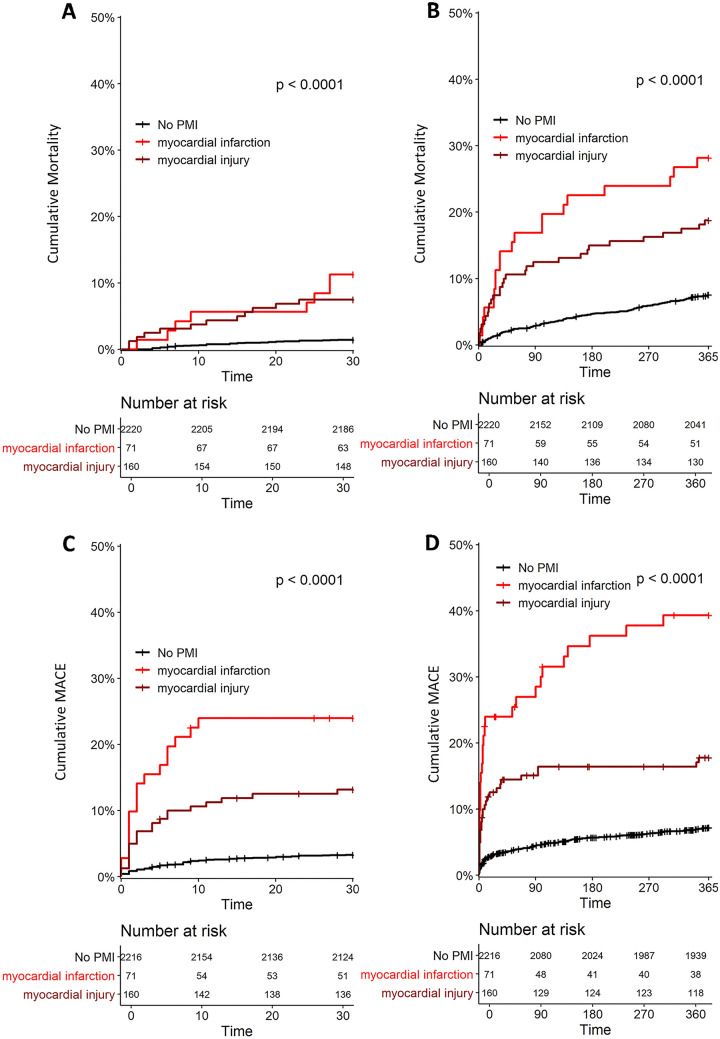
Methods: We prospectively included 2455 patients at high cardiovascular risk undergoing 3111 non-cardiac surgeries, for whom hs-cTnI and hs-cTnT concentrations were measured before surgery and on postoperative days 1 and 2. PMI was defined as a composite of perioperative myocardial infarction (PMIInfarct) and perioperative myocardial injury (PMIInjury), according to the Fourth Universal Definition of Myocardial Infarction. All-cause mortality was the primary endpoint.
Results: Using hs-cTnI, the incidence of overall PMI was 9% (95% confidence interval [CI] 8-10%), including PMIInfarct 2.6% (95% CI 2.0-3.2) and PMIInjury 6.1% (95% CI 5.3-6.9%), which was lower versus using hs-cTnT: overall PMI 15% (95% CI 14-16%), PMIInfarct 3.7% (95% CI 3.0-4.4) and PMIInjury 11.3% (95% CI 10.2-12.4%). All-cause mortality occurred in 52 (2%) patients within 30 days and 217 (9%) within 1 year. Using hs-cTnI, both PMIInfarct and PMIInjury were independent predictors of 30-day all-cause mortality (adjusted hazard ratio [aHR] 2.5 [95% CI 1.1-6.0], and aHR 2.8 [95% CI 1.4-5.5], respectively) and, 1-year all-cause mortality (aHR 2.0 [95% CI 1.2-3.3], and aHR 1.8 [95% CI 1.2-2.7], respectively). Overall, the prognostic impact of PMI diagnosed by hs-cTnI was comparable to the prognostic impact of PMI using hs-cTnT.
Conclusions: Using hs-cTnI, PMI is less common versus using hs-cTnT. Using hs-cTnI, both PMIInfarct and PMIInjury remain independent predictors of 30-day and 1-year mortality.
Keywords: High-sensitivity troponin; Myocardial infarction; Myocardial injury; Non-cardiac surgery; Perioperative care.
© 2021. The Author(s).
Conflict of interest statement
Dr. Gualandro reports grants from FAPESP (Fundacao de Amparo a pesquisa do estado de Sao Paulo; Brasil); during the conduct of the study; personal fees from Roche; outside the submitted work; Dr. Puelacher reports grants from PhD Educational Platform for Health Sciences; grants from Roche Diagnostics; grants from University Hospital Basel; during the conduct of the study; other from Roche; outside the submitted work; Dr. Lurati Buse reports grants from University of Basel; during the conduct of the study; other from Roche Diagnostic; outside the submitted work; Dr. Cardozo reports personal fees from Bayer; outside the submitted work; Dr. Arslani reports grants from Swiss Academy of Medical Siences and the Bangerter Foundation; outside the submitted work; Dr. Calderaro reports personal fees from Bayer; personal fees from Janssen; personal fees from Daiichi Sankyo; from null; outside the submitted work; Dr. Hammerer-Lercher reports other from Roche Diagnostics; other from Abbott Diagnostics; other from Beckman Diagnostics; outside the submitted work; Dr. Kindler reports grants from Research Fund Kantonsspital Aarau; during the conduct of the study; Dr. Osswald reports grants from SNSF for Swiss-AF cohort study; outside the submitted work; Dr. Devereaux is a member of a research group with a policy of not accepting honorariums or other payments from industry for their own personal financial gain. They do accept honorariums/payments from industry to support research endeavours and costs to participate in meetings. Based on study questions he has originated and grants he has written; he has received grants from Abbott Diagnostics; AstraZeneca; Bayer; Boehringer Ingelheim; Bristol-Myers-Squibb; Coviden; Octapharma; Philips Healthcare; Roche Diagnostics and Stryker. Dr. Mueller has received research support/grants from the Swiss National Science Foundation, the Swiss Heart Foundation, the Cardiovascular Research Foundation Basel, the University Hospital Basel, the University of Basel, Abbott, Beckman Coulter, BRAHMS, Ortho Clinical, Quidel, Roche, Siemens, and Sphingotec, as well as speaker/consulting honoraria from Acon, Amgen, Astra Zeneca, Bayer, Boehringer Ingelheim, Osler, Novartis, Roche, and Sanofi. All other authors have no conflict of interest to declare.
Figures


References
-
- Puelacher C, Lurati Buse G, Seeberger D, Sazgary L, Marbot S, Lampart A, Espinola J, Kindler C, Hammerer A, Seeberger E, Strebel I, Wildi K, Twerenbold R, du Fay de Lavallaz J, Steiner L, Gurke L, Breidthardt T, Rentsch K, Buser A, Gualandro DM, Osswald S, Mueller C. Perioperative myocardial injury after noncardiac surgery: incidence, mortality, and characterization. Circulation. 2018;137(12):1221–1232. doi: 10.1161/CIRCULATIONAHA.117.030114. - DOI - PubMed
-
- Devereaux PJ, Biccard BM, Sigamani A, Xavier D, Chan MTV, Srinathan SK, Walsh M, Abraham V, Pearse R, Wang CY, Sessler DI, Kurz A, Szczeklik W, Berwanger O, Villar JC, Malaga G, Garg AX, Chow CK, Ackland G, Patel A, Borges FK, Belley-Cote EP, Duceppe E, Spence J, Tandon V, Williams C, Sapsford RJ, Polanczyk CA, Tiboni M, Alonso-Coello P, Faruqui A, Heels-Ansdell D, Lamy A, Whitlock R, LeManach Y, Roshanov PS, McGillion M, Kavsak P, McQueen MJ, Thabane L, Rodseth RN, Buse GAL, Bhandari M, Garutti I, Jacka MJ, Schünemann HJ, Cortes OL, Coriat P, Dvirnik N, Botto F, Pettit S, Jaffe AS, Guyatt GH. Association of postoperative high-sensitivity troponin levels with myocardial injury and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2017;317(16):1642–1651. doi: 10.1001/jama.2017.4360. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
