

Multicatheter interstitial brachytherapy versus stereotactic radiotherapy with CyberKnife for accelerated partial breast irradiation: a comparative treatment planning study with respect to dosimetry of organs at risk
- PMID: 33768766
- PMCID: PMC8042824
- DOI: 10.2478/raon-2021-0016
Multicatheter interstitial brachytherapy versus stereotactic radiotherapy with CyberKnife for accelerated partial breast irradiation: a comparative treatment planning study with respect to dosimetry of organs at risk
Abstract
Background: The aim of the study was to dosimetrically compare multicatheter interstitial brachytherapy (MIBT) and stereotactic radiotherapy with CyberKnife (CK) for accelerated partial breast irradiation (APBI) especially concerning the dose of organs at risk (OAR-s).
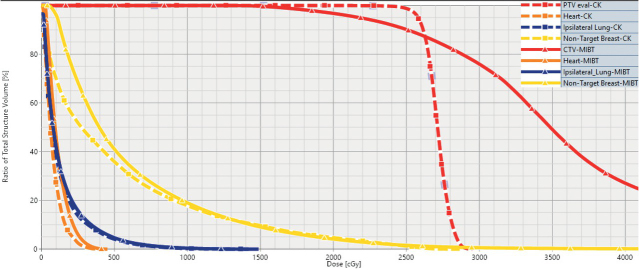
Patients and methods: Treatment plans of thirty-two MIBT and CK patients were compared. The OAR-s included ipsilateral non-target and contralateral breast, ipsilateral and contralateral lung, skin, ribs, and heart for left-sided cases. The fractionation was identical (4 x 6.25 Gy) in both treatment groups. The relative volumes (e.g. V100, V90) receiving a given relative dose (100%, 90%), and the relative doses (e.g. D0.1cm3, D1cm3) delivered to the most exposed small volumes (0.1 cm3, 1 cm3) were calculated from dose-volume histograms. All dose values were related to the prescribed dose (25 Gy).
Results: Regarding non-target breast CK performed slightly better than MIBT (V100: 0.7% vs. 1.6%, V50: 10.5% vs. 12.9%). The mean dose of the ipsilateral lung was the same for both techniques (4.9%), but doses irradiated to volume of 1 cm3 were lower with MIBT (36.1% vs. 45.4%). Protection of skin and rib was better with MIBT. There were no significant differences between the dose-volume parameters of the heart, but with MIBT, slightly larger volumes were irradiated by 5% dose (V5: 29.9% vs. 21.2%). Contralateral breast and lung received a somewhat higher dose with MIBT (D1cm3: 2.6% vs. 1.8% and 3.6% vs. 2.5%).
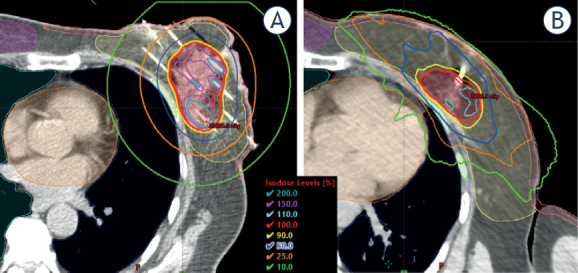
Conclusions: The target volume can be properly irradiated by both techniques with similar dose distributions and high dose conformity. Regarding the dose to the non-target breast, heart, and contralateral organs the CK was superior, but the nearby organs (skin, ribs, ipsilateral lung) received less dose with MIBT. The observed dosimetric differences were small but significant in a few parameters at the examined patient number. More studies are needed to explore whether these dosimetric findings have clinical significance.
Keywords: APBI; CyberKnife; dosimetric comparison; multicatheter interstitial brachytherapy.
© 2021 András Herein, Gábor Stelczer, Csilla Pesznyák, Georgina Fröhlich, Viktor Smanykó, Norbert Mészáros, Csaba Polgár, Tibor Major, published by Sciendo.
Figures
Similar articles
-
Multicatheter interstitial brachytherapy versus intensity modulated external beam therapy for accelerated partial breast irradiation: A comparative treatment planning study with respect to dosimetry of organs at risk.Radiother Oncol. 2017 Jan;122(1):17-23. doi: 10.1016/j.radonc.2016.08.003. Epub 2016 Aug 17. Radiother Oncol. 2017. PMID: 27544819
-
CyberKnife versus multicatheter interstitial brachytherapy for accelerated partial breast irradiation: a dosimetrical assessment with focus on organs at risk.Rep Pract Oncol Radiother. 2022 Mar 22;27(1):152-160. doi: 10.5603/RPOR.a2022.0011. eCollection 2022. Rep Pract Oncol Radiother. 2022. PMID: 35402040 Free PMC article.
-
Dosimetric analysis of breast cancer tumor bed boost: An interstitial brachytherapy vs. external beam radiation therapy comparison for deeply seated tumors.Brachytherapy. 2020 Mar-Apr;19(2):264-274. doi: 10.1016/j.brachy.2019.10.008. Epub 2019 Nov 29. Brachytherapy. 2020. PMID: 31787575
-
American Brachytherapy Society consensus report for accelerated partial breast irradiation using interstitial multicatheter brachytherapy.Brachytherapy. 2017 Sep-Oct;16(5):919-928. doi: 10.1016/j.brachy.2017.05.012. Epub 2017 Jul 1. Brachytherapy. 2017. PMID: 28676428 Review.
-
Accelerated partial breast irradiation by brachytherapy: present evidence and future developments.Jpn J Clin Oncol. 2020 Jul 9;50(7):743-752. doi: 10.1093/jjco/hyaa064. Jpn J Clin Oncol. 2020. PMID: 32444872 Review.
Cited by
-
Low doses to the heart in daily practice for treating left-sided breast cancer using accelerated partial-breast irradiation by multicatheter brachytherapy and deep-inspiration breath-hold using a SIB.Strahlenther Onkol. 2023 Apr;199(4):389-395. doi: 10.1007/s00066-023-02047-z. Epub 2023 Feb 24. Strahlenther Onkol. 2023. PMID: 36826517 Free PMC article.
-
Post- versus intra-operative implant for breast cancer interstitial brachytherapy: How to choose?J Contemp Brachytherapy. 2024 Feb;16(1):72-83. doi: 10.5114/jcb.2024.135635. Epub 2024 Feb 23. J Contemp Brachytherapy. 2024. PMID: 38584881 Free PMC article.
-
External Beam Accelerated Partial Breast Irradiation in Early Breast Cancer and the Risk for Radiogenic Pneumonitis.Cancers (Basel). 2022 Jul 20;14(14):3520. doi: 10.3390/cancers14143520. Cancers (Basel). 2022. PMID: 35884579 Free PMC article.
-
Stereotactic body radiotherapy using CyberKnife versus interstitial brachytherapy in accelerated partial breast irradiation on left-sided breast: A comparison of dosimetric characteristics and preliminary clinical results.Breast. 2024 Dec;78:103796. doi: 10.1016/j.breast.2024.103796. Epub 2024 Sep 4. Breast. 2024. PMID: 39243564 Free PMC article.
-
Interstitial High-Dose-Rate Brachytherapy Combined with External Beam Radiation Therapy for Dose Escalation in the Primary Treatment of Locally Advanced, Non-Resectable Superior Sulcus (Pancoast) Tumors: Results of a Monocentric Retrospective Study.J Clin Med. 2024 Dec 11;13(24):7550. doi: 10.3390/jcm13247550. J Clin Med. 2024. PMID: 39768473 Free PMC article.
References
-
- Darby S, Mc Gale P, Correa C, Taylor C, Arriagada R, Clarke M. Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis on individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378:1707–16. doi: 10.1016/S0140-6736(11)61629-2. et al. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials