

Case Reports
doi: 10.1002/ccr3.3836.
eCollection 2021 Mar.
Overlapping holoprosencephaly-polydactyl syndrome and asphyxiating thoracic dystrophy, an incidental finding in late prenatal ultrasound: A rare case report
Affiliations
- PMID: 33768892
- PMCID: PMC7981735
- DOI: 10.1002/ccr3.3836
Item in Clipboard
Case Reports
Overlapping holoprosencephaly-polydactyl syndrome and asphyxiating thoracic dystrophy, an incidental finding in late prenatal ultrasound: A rare case report
Clin Case Rep.
.
Abstract
Holoprosencephaly-polydactyly syndrome and asphyxiating thoracic dystrophy rarely overlap but if they do, they have poorer prognosis. Early prenatal detection of multiple congenital anomalies plays a crucial role in the management of pregnancy.
Keywords: Jeune syndrome; alobar holoprosencephaly; polydactyl; short ribs.
© 2021 The Authors. Clinical Case Reports published by John Wiley & Sons Ltd.
Conflict of interest statement
None declare.
Figures

(A, B (1,2), C, D, E and F) – prenatal ultrasound. A, Demonstrates absence of midline structures and single ventricle, head circumference (377 mm) and biparietal diameter (114 mm) below > 95th percentile for gestational age. B1, Demonstrates abdominal circumference (283 mm) which was between 10th and 50th percentile, double bubble sign, B2, Narrow chest (Chest circumference = 170 mm), short and horizontal ribs which was <5th percentile. C, Color Doppler demonstrates no flow in the remained brain parenchyma and three‐vessel cord of umbilicus. D, Demonstrates absence of nasal bone. E, Demonstrates short radius (10.7 mm) and ulna (10.3 mm) which was <5th percentile. F, Demonstrates very short femur (FL = 16.5 mm) which was <5th percentile

(A, B and C) post‐delivery images of the neonate. A phenotypically female neonate with big head, flat nose, low set ears, small chest, invariably short limbs,and polydactyly of four limbs
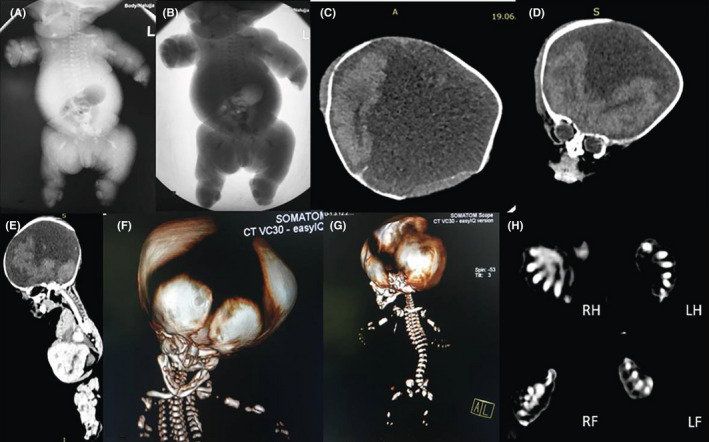
(A and B) postnatal radiography study. (C, D, and E) CT scan with brain window. (F and G) 3D CT bone reformat. (H) CT scan in bone window. (A and B) demonstrate short and horizontal oriented ribs, bilateral short humerus, and femur. (C, D and E) demonstrate absent midline structures with frontal lobes and occipital lobe in place. F) Demonstrates widely open cranial sutures. (G) Demonstrates short and horizontally oriented ribs. (H) demonstrates postaxial polydactyly of the Right hand (RH), Left hand (LH), Right foot (RF), and Left foot (LF)
References
-
- DeMyer W, Zeman W, Palmer CG. The face predicts the brain: diagnostic significance of median facial anomalies for holoprosencephaly (arhinencephaly). Pediatrics. 1963;34:256‐263. - PubMed
-
- Cedrik T‐N, Maximilian M, Paul K. Holoprosencephaly overview. In: Adam MP, Ardinger HH, Pagon RA, et al. GeneReviews®. Seattle, WA: University of Washington; 2000.
-
- Li‐Hsiung C. Alobar holoprosencephaly: report of two cases with unusual findings. Chang Gung Med J. 2003;26(9):700‐776. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
