

Updated strategies in the management of acute variceal haemorrhage
- PMID: 33769373
- PMCID: PMC8691141
- DOI: 10.1097/MOG.0000000000000723
Updated strategies in the management of acute variceal haemorrhage
Abstract
Purpose of review: This article reviews the most recent studies regarding the management of acute esophageal variceal haemorrhage.
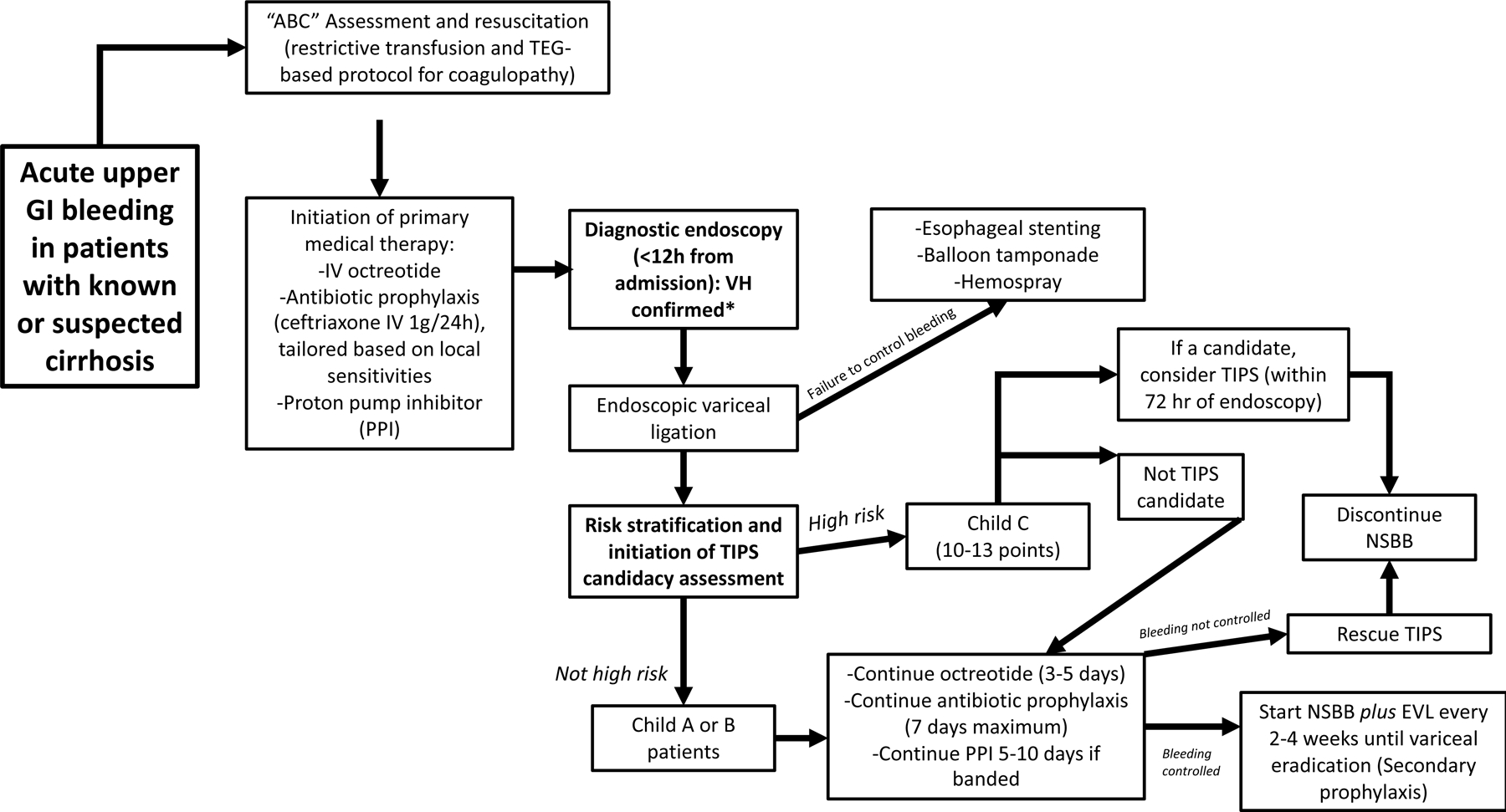
Recent findings: New randomized control trials and meta-analyses confirmed the role of early transjugular intrahepatic portosystemic shunt (TIPS) in the management of acute variceal haemorrhage in Child-Pugh C (10-13) and B patients with active bleeding. A recent randomized controlled trial focused on the duration of vasoactive therapy showed no difference between 2 and 5 days of octreotide. A randomized trial showed decreased use of blood products for the correction of coagulopathy using a thromboelastography-guided approach (vs. conventional parameters) as well as decreased bleeding rates when compared with standard of care. A meta-analysis found that for rescue of variceal bleeding, self-expanding metallic stents were more efficacious and safer than balloon tamponade. In addition, studies showed that Child-Pugh C patients and those with hepatic vein pressure gradient more than 20 were at the highest risk of treatment failure, while model for end-stage liver disease was highly predictive of in-hospital mortality.
Summary: In patients with severe coagulopathy and uncontrolled bleeding, TEG-based transfusion strategies are recommended. Antibiotics should be used for all cirrhotic patients presenting with upper gastrointestinal bleeding, but should be tailored in accordance to local resistance patterns. Early TIPS for high-risk patients has been shown to have a significant survival benefit. Certain aspects of the management of variceal bleeding remain poorly studied such as the role of early TIPS in Child-B patients as well as strategies for rescue therapy in patients who are not TIPS candidates, and require further investigation.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Early TIPS with covered stents versus standard treatment for acute variceal bleeding in patients with advanced cirrhosis: a randomised controlled trial.Lancet Gastroenterol Hepatol. 2019 Aug;4(8):587-598. doi: 10.1016/S2468-1253(19)30090-1. Epub 2019 May 29. Lancet Gastroenterol Hepatol. 2019. PMID: 31153882 Clinical Trial.
-
Endoscopic diagnosis and management of esophagogastric variceal hemorrhage: European Society of Gastrointestinal Endoscopy (ESGE) Guideline.Endoscopy. 2022 Nov;54(11):1094-1120. doi: 10.1055/a-1939-4887. Epub 2022 Sep 29. Endoscopy. 2022. PMID: 36174643
-
Model for end-stage liver disease score and hemodynamic instability as a predictor of poor outcome in early transjugular intrahepatic portosystemic shunt treatment for acute variceal hemorrhage.Eur J Gastroenterol Hepatol. 2018 Dec;30(12):1441-1446. doi: 10.1097/MEG.0000000000001222. Eur J Gastroenterol Hepatol. 2018. PMID: 30048333
-
Current approaches to the management of patients with liver cirrhosis who have acute esophageal variceal bleeding.Curr Med Res Opin. 2016;32(3):467-75. doi: 10.1185/03007995.2015.1124846. Epub 2016 Jan 25. Curr Med Res Opin. 2016. PMID: 26804426 Review.
-
Early transjugular intrahepatic portosystemic shunt for acute variceal bleeding: a systematic review and meta-analysis.Eur Radiol. 2021 Jul;31(7):5390-5399. doi: 10.1007/s00330-020-07525-x. Epub 2021 Jan 6. Eur Radiol. 2021. PMID: 33409783
Cited by
-
Emergency Endoscopic Interventions in Acute Upper Gastrointestinal Bleeding: A Cohort Study.Diagnostics (Basel). 2023 Dec 1;13(23):3584. doi: 10.3390/diagnostics13233584. Diagnostics (Basel). 2023. PMID: 38066825 Free PMC article.
-
Role of Interventional Radiology (IR) in vascular emergencies among cirrhotic patients.Emerg Radiol. 2024 Feb;31(1):83-96. doi: 10.1007/s10140-023-02184-z. Epub 2023 Nov 17. Emerg Radiol. 2024. PMID: 37978126 Review.
-
[Current Interventional Management of Acute Upper Gastrointestinal Bleeding].Sichuan Da Xue Xue Bao Yi Xue Ban. 2022 May;53(3):361-366. doi: 10.12182/20220560206. Sichuan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 35642139 Free PMC article. Review. Chinese.
-
[Outcomes of Endoscopic Treatment of Esophagogastric Variceal Bleeding and Construction and Validation of a 1-Year Rebleeding Risk Prediction Model].Sichuan Da Xue Xue Bao Yi Xue Ban. 2025 Jan 20;56(1):284-290. doi: 10.12182/20250160106. Sichuan Da Xue Xue Bao Yi Xue Ban. 2025. PMID: 40109450 Free PMC article. Chinese.
-
Innovative Strategies in the Diagnosis and Treatment of Liver Cirrhosis and Associated Syndromes.Life (Basel). 2025 May 13;15(5):779. doi: 10.3390/life15050779. Life (Basel). 2025. PMID: 40430206 Free PMC article. Review.
References
-
- de Franchis R, Primignani M. Natural History of Portal Hypertension in Patients with Cirrhosis. Clinics in Liver Disease 2001;5(3):645–663. - PubMed
-
- Kovalak M, Lake J, Mattek N, Eisen G, Lieberman D, Zaman A. Endoscopic screening for varices in cirrhotic patients: data from a national endoscopic database. Gastrointest Endosc 2007;65(1):82–88. - PubMed
-
- Garcia-Tsao G, Abraldes JG, Berzigotti A, Bosch J. Portal hypertensive bleeding in cirrhosis: Risk stratification, diagnosis, and management: 2016 practice guidance by the American Association for the study of liver diseases. Hepatology 2017;65(1):310–335. - PubMed
-
- Reverter E, Tandon P, Augustin S, et al. A MELD-based model to determine risk of mortality among patients with acute variceal bleeding. Gastroenterology 2014;146(2):412–419 e413. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
