

Why translation from basic discoveries to clinical applications is so difficult for atrial fibrillation and possible approaches to improving it
- PMID: 33769493
- PMCID: PMC8208745
- DOI: 10.1093/cvr/cvab093
Why translation from basic discoveries to clinical applications is so difficult for atrial fibrillation and possible approaches to improving it
Abstract
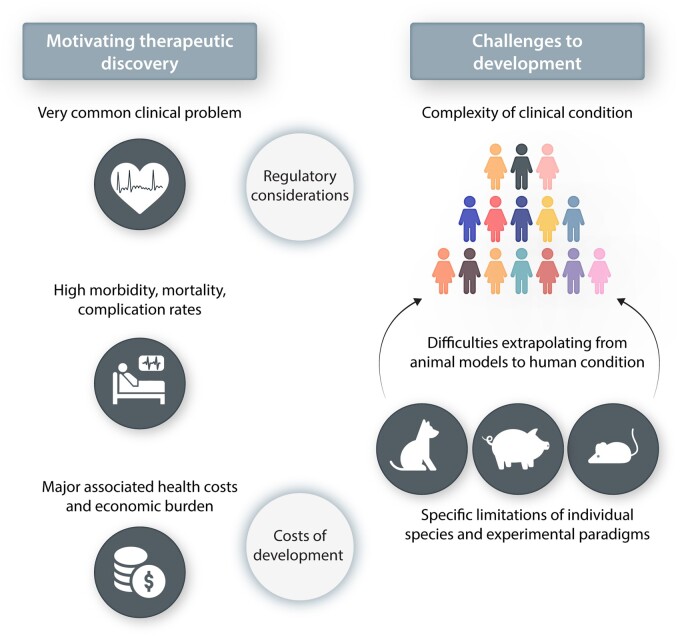
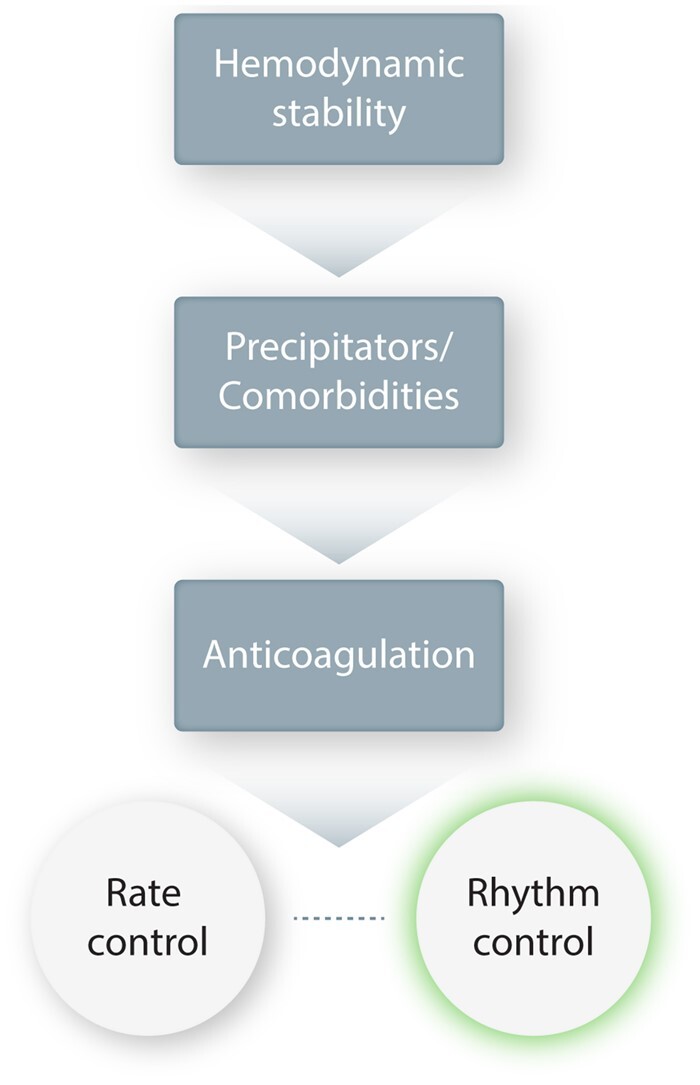
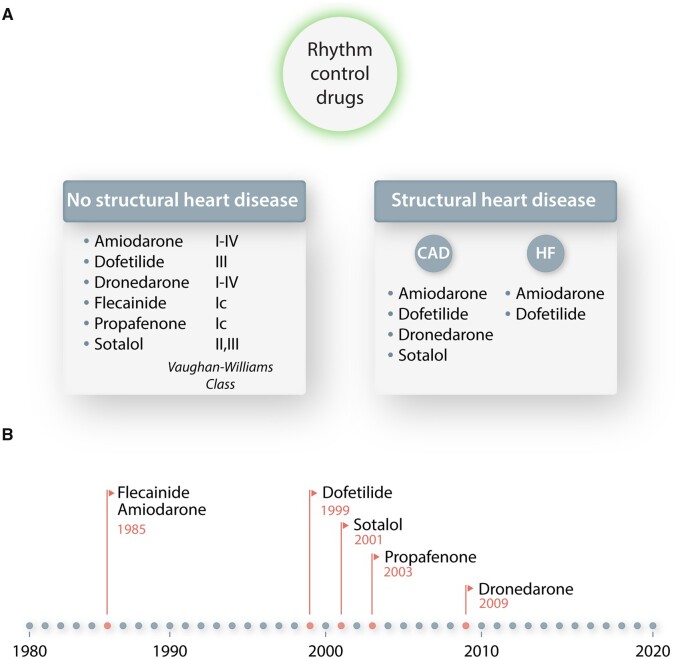
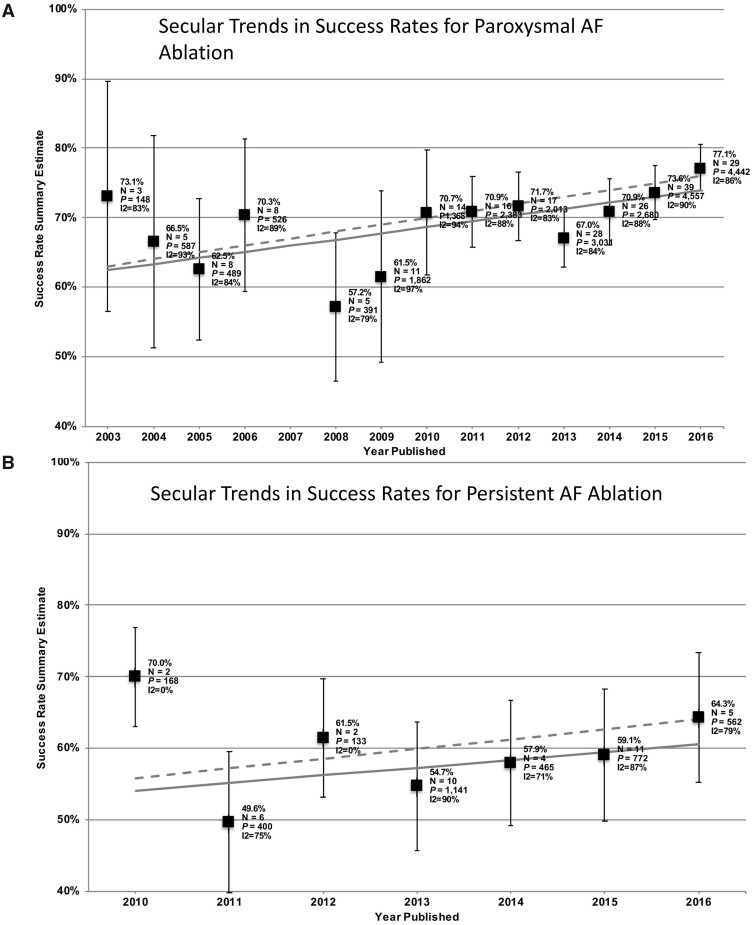
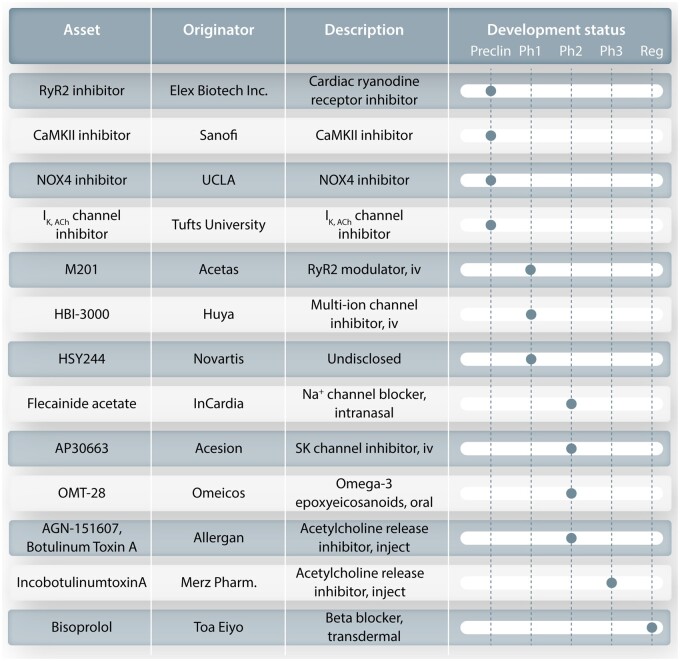
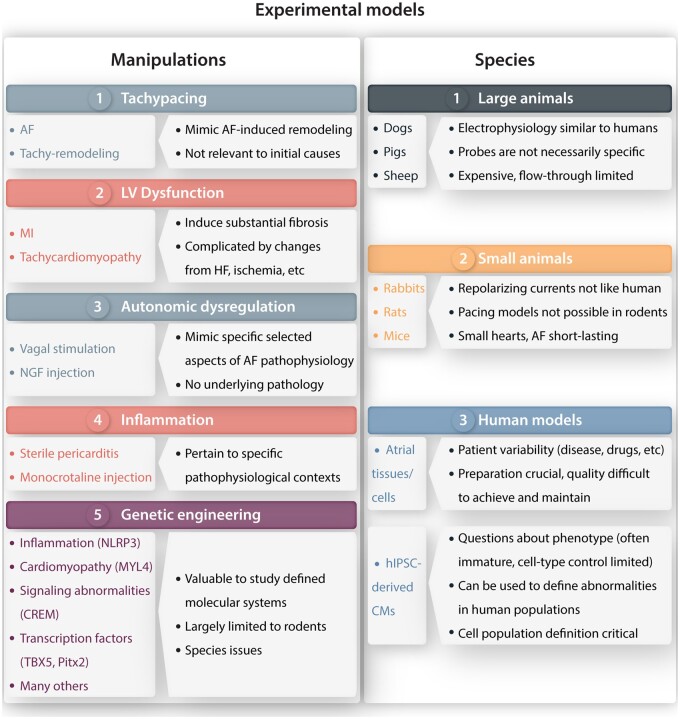
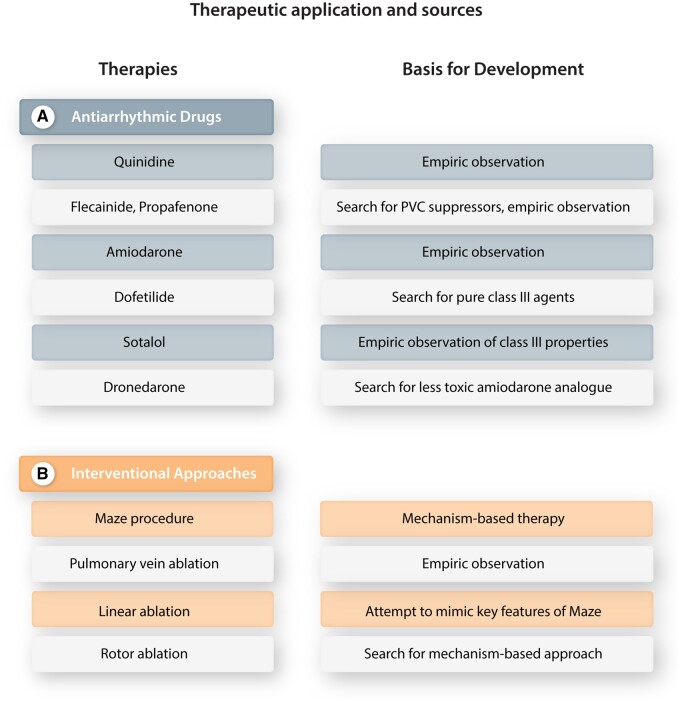
Atrial fibrillation (AF) is the most common sustained clinical arrhythmia, with a lifetime incidence of up to 37%, and is a major contributor to population morbidity and mortality. Important components of AF management include control of cardiac rhythm, rate, and thromboembolic risk. In this narrative review article, we focus on rhythm-control therapy. The available therapies for cardiac rhythm control include antiarrhythmic drugs and catheter-based ablation procedures; both of these are presently neither optimally effective nor safe. In order to develop improved treatment options, it is necessary to use preclinical models, both to identify novel mechanism-based therapeutic targets and to test the effects of putative therapies before initiating clinical trials. Extensive research over the past 30 years has provided many insights into AF mechanisms that can be used to design new rhythm-maintenance approaches. However, it has proven very difficult to translate these mechanistic discoveries into clinically applicable safe and effective new therapies. The aim of this article is to explore the challenges that underlie this phenomenon. We begin by considering the basic problem of AF, including its clinical importance, the current therapeutic landscape, the drug development pipeline, and the notion of upstream therapy. We then discuss the currently available preclinical models of AF and their limitations, and move on to regulatory hurdles and considerations and then review industry concerns and strategies. Finally, we evaluate potential paths forward, attempting to derive insights from the developmental history of currently used approaches and suggesting possible paths for the future. While the introduction of successful conceptually innovative new treatments for AF control is proving extremely difficult, one significant breakthrough is likely to revolutionize both AF management and the therapeutic development landscape.
Keywords: Antiarrhythmic drugs; Atrial fibrillation; Mechanisms; Personalized therapy; Remodelling.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2021. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Du X, Dong J, Ma C. Is atrial fibrillation a preventable disease? J Am Coll Cardiol 2017;69:1968–1982. - PubMed
-
- Kannel WB, Wolf PA, Benjamin EJ, Levy D. Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol 1998;82:2N–9N. - PubMed
-
- Wang TJ, Larson MG, Levy D, Vasan RS, Leip EP, Wolf PA, D'Agostino RB, Murabito JM, Kannel WB, Benjamin EJ. Temporal relations of atrial fibrillation and congestive heart failure and their joint influence on mortality: the Framingham Heart Study. Circulation 2003;107:2920–2925. - PubMed
-
- Kim MH, Johnston SS, Chu BC, Dalal MR, Schulman KL. Estimation of total incremental health care costs in patients with atrial fibrillation in the United States. Circ Cardiovasc Qual Outcomes 2011;4:313–320. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
