

Risk factors for in-hospital mortality in laboratory-confirmed COVID-19 patients in the Netherlands: A competing risk survival analysis
- PMID: 33770140
- PMCID: PMC7997038
- DOI: 10.1371/journal.pone.0249231
Risk factors for in-hospital mortality in laboratory-confirmed COVID-19 patients in the Netherlands: A competing risk survival analysis
Abstract
Background: To date, survival data on risk factors for COVID-19 mortality in western Europe is limited, and none of the published survival studies have used a competing risk approach. This study aims to identify risk factors for in-hospital mortality in COVID-19 patients in the Netherlands, considering recovery as a competing risk.
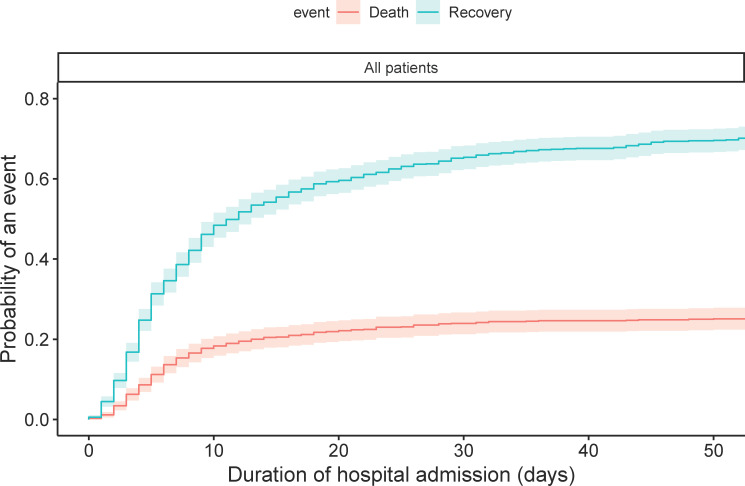
Methods: In this observational multicenter cohort study we included adults with PCR-confirmed SARS-CoV-2 infection that were admitted to one of five hospitals in the Netherlands (March to May 2020). We performed a competing risk survival analysis, presenting cause-specific hazard ratios (HRCS) for the effect of preselected factors on the absolute risk of death and recovery.
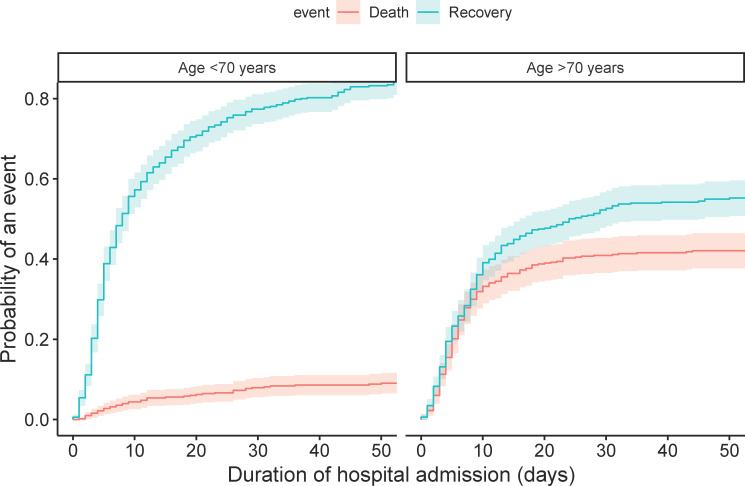
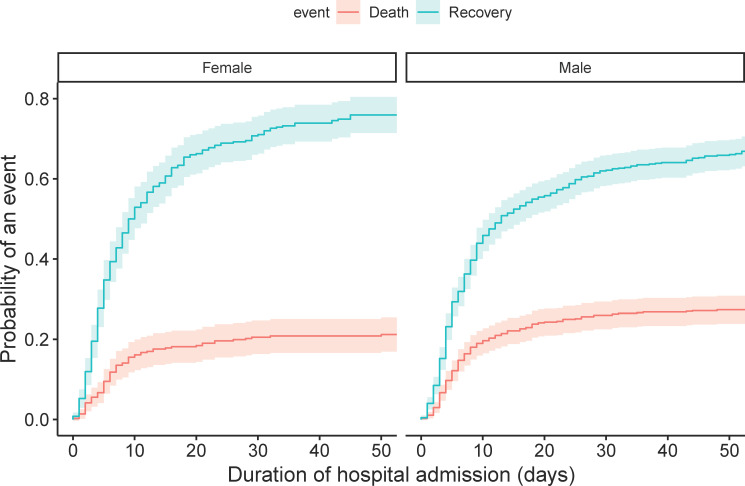
Results: 1,006 patients were included (63.9% male; median age 69 years, IQR: 58-77). Patients were hospitalized for a median duration of 6 days (IQR: 3-13); 243 (24.6%) of them died, 689 (69.9%) recovered, and 74 (7.4%) were censored. Patients with higher age (HRCS 1.10, 95% CI 1.08-1.12), immunocompromised state (HRCS 1.46, 95% CI 1.08-1.98), who used anticoagulants or antiplatelet medication (HRCS 1.38, 95% CI 1.01-1.88), with higher modified early warning score (MEWS) (HRCS 1.09, 95% CI 1.01-1.18), and higher blood LDH at time of admission (HRCS 6.68, 95% CI 1.95-22.8) had increased risk of death, whereas fever (HRCS 0.70, 95% CI 0.52-0.95) decreased risk of death. We found no increased mortality risk in male patients, high BMI or diabetes.
Conclusion: Our competing risk survival analysis confirms specific risk factors for COVID-19 mortality in a the Netherlands, which can be used for prediction research, more intense in-hospital monitoring or prioritizing particular patients for new treatments or vaccination.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Dutch National Institute for Public Health and the Environment (RIVM). Patient with novel coronavirus COVID-19 in the Netherlands 2020 [updated 27-02-2020. Available from: https://www.rivm.nl/en/news/patient-with-novel-coronavirus-covid-19-in-n....
-
- Dutch National Institute for Public Health and the Environment (RIVM). Current information about the novel coronavirus (COVID-19) 2020 [updated 06-04-2020. Available from: https://www.rivm.nl/en/current-information-about-novel-coronavirus-covid-19.
-
- World Health Organization (WHO. Coronavirus (COVID-19), global situation dashboard: WHO; 2020. [Available from: https://covid19.who.int/.
-
- Schuster NA, Hoogendijk EO, Kok AAL, Twisk JWR, Heymans MW. Ignoring competing events in the analysis of survival data may lead to biased results: a nonmathematical illustration of competing risk analysis. Journal of clinical epidemiology. 2020;122:42–8. 10.1016/j.jclinepi.2020.03.004 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
