

Detection methods for SARS-CoV-2 in tissue
- PMID: 33770236
- PMCID: PMC7994356
- DOI: 10.1007/s00292-021-00920-1
Detection methods for SARS-CoV-2 in tissue
Abstract
Background: Analyses for the presence of SARS-CoV‑2 in the tissues of COVID-19 patients is important in order to improve our understanding of the disease pathophysiology for interpretation of diagnostic histopathological findings in autopsies, biopsies, or surgical specimens and to assess the potential for occupational infectious hazard.
Material and methods: In this review we identified 136 published studies in PubMed's curated literature database LitCovid on SARS-CoV‑2 detection methods in tissues and evaluated them regarding sources of error, specificity, and sensitivity of the methods, taking into account our own experience.
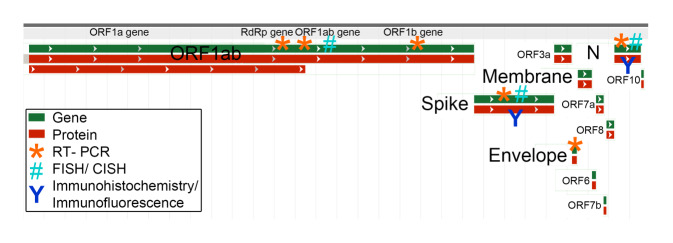
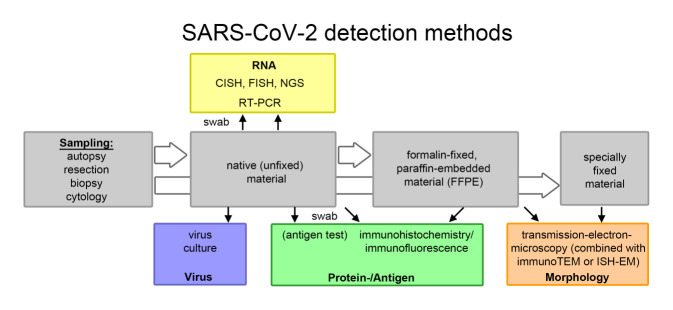
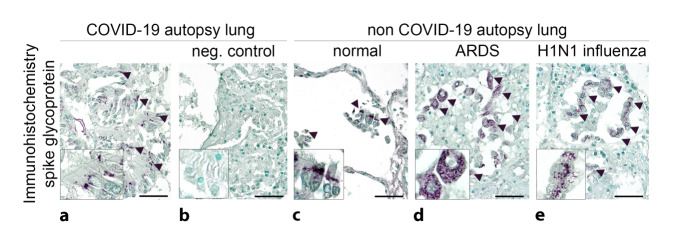
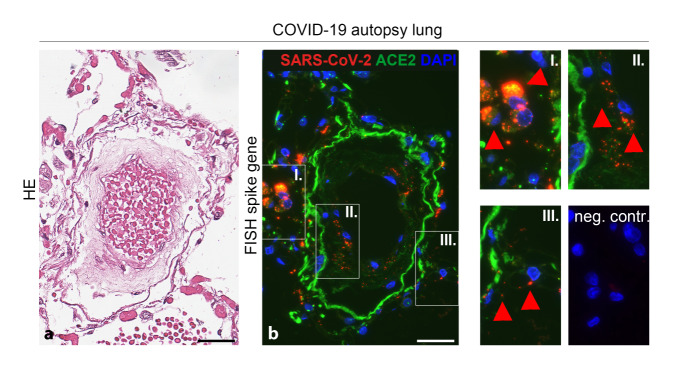
Results: Currently, no sufficiently specific histomorphological alterations or diagnostic features for COVID-19 are known. Therefore, three approaches for SARS-CoV‑2 detection are used: RNA, proteins/antigens, or morphological detection by electron microscopy. In the preanalytical phase, the dominant source of error is tissue quality, especially the different intervals between sample collection and processing or fixation (and its duration) and specifically the interval between death and sample collection in autopsies. However, this information is found in less than half of the studies (e.g., in only 42% of autopsy studies). Our own experience and first studies prove the significantly higher sensitivity and specificity of RNA-based detection methods compared to antigen or protein detection by immunohistochemistry or immunofluorescence. Detection by electron microscopy is time consuming and difficult to interpret.
Conclusions: Different methods are available for the detection of SARS-CoV‑2 in tissue. Currently, RNA detection by RT-PCR is the method of choice. However, extensive validation studies and method harmonization are not available and are absolutely necessary.
Zusammenfassung: HINTERGRUND: Die Analyse von SARS-CoV‑2 in Geweben von COVID-19-Patienten ist wichtig für ein besseres Verständnis der Pathophysiologie der Krankheit, die Interpretation der diagnostischen histopathologischen Befunde in Autopsien, Biopsien und Resektaten oder um ein potenzielles berufsbedingtes Infektionsrisiko einzuschätzen.
Material und methoden: In dieser Übersichtsarbeit haben wir 136 publizierte Studien zu Detektionsmethoden von SARS-CoV‑2 in Gewebe in der kuratierten Literaturdatenbank LitCovid von PubMed identifiziert und bezüglich Fehlerquellen, Spezifität und Sensitivität der Methoden unter Berücksichtigung eigener Erfahrungen ausgewertet.
Ergebnisse: Es gibt keine ausreichend spezifischen histomorphologischen Veränderungen bzw. diagnostischen Merkmale von COVID-19. Daher werden 3 Ansätze zum SARS-CoV-2-Nachweis genutzt: Nachweis von RNA, Proteinen/Antigenen oder morphologischer Nachweis mittels Elektronenmikroskopie. In der präanalytischen Phase liegt die dominante Fehlerquelle in der Gewebequalität, insbesondere den unterschiedlichen Intervallen zwischen Probenentnahme und -aufarbeitung, sowie spezifisch in Autopsien im Intervall zwischen Tod und Probenentnahme. Diese Angaben finden sich in weniger als der Hälfte der Studien (z. B. nur in 42 % der Autopsiestudien). Eigene Erfahrungen und erste Studien belegen die deutlich höhere Sensitivität und Spezifität von RNA-basierten Nachweismethoden gegenüber Antigen- bzw. Proteinnachweis mittels Immunhistochemie oder Immunfluoreszenz. Der Nachweis mittels Elektronenmikroskopie ist zeitintensiv und die Interpretation schwierig.
Schlussfolgerungen: Es stehen verschiedene Methoden zum Nachweis von SARS-CoV‑2 im Gewebe zur Verfügung. Derzeit ist der RNA-Nachweis mittels RT-PCR die Methode der Wahl. Notwendige, umfangreiche Validationsstudien und Methodenharmonisierung sind derzeit noch nicht verfügbar.
Keywords: COVID-19; Electron microscopy; Fluorescence in situ hybridization; Preanalytical phase; Reverse transcriptase polymerase chain reaction.
© 2021. Springer Medizin Verlag GmbH, ein Teil von Springer Nature.
Conflict of interest statement
S. von Stillfried and P. Boor declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
