

Cost effectiveness of outpatient lumbar discectomy
- PMID: 33771175
- PMCID: PMC8004396
- DOI: 10.1186/s12962-021-00272-w
Cost effectiveness of outpatient lumbar discectomy
Abstract
Background: Microdiscectomy is the most commonly performed spine surgery and the first transitioning for outpatient settings. However, this transition was never studied, in what comes to cost-utility assessment. Accordingly, this economic study aims to access the cost-effectiveness of outpatient lumbar microdiscectomy when compared with the inpatient procedure.
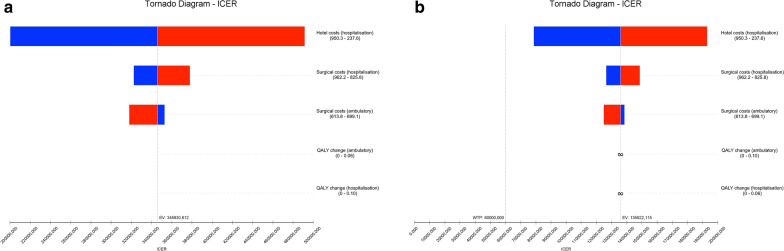
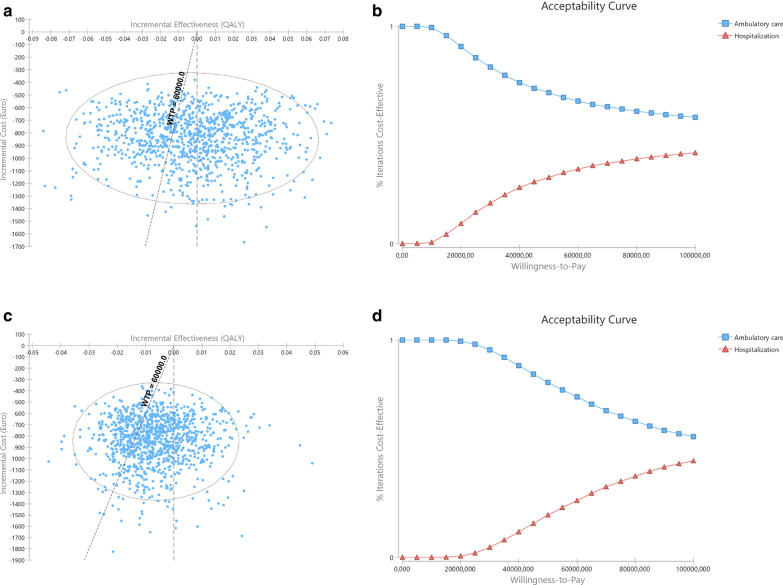
Methods: This is a cost utility study, adopting the hospital perspective. Direct medical costs were retrieved from the assessment of 20 patients undergoing outpatient lumbar microdiscectomy and 20 undergoing inpatient lumbar microdiscectomy Quality-adjusted life-years were calculated from Oswestry Disability Index values (ODI). ODI was prospectively assessed in outpatients in pre and 3- and 6-month post-operative evaluations. Inpatient ODI data were estimated from a meta-analysis. A probabilistic sensitivity analysis was performed and incremental cost-effectiveness ratio (ICER) calculated.
Results: Outpatient procedure was cost-saving in all models tested. At 3-month assessment ICER ranged from €135,753 to €345,755/QALY, higher than the predefined threshold of €60,000/QALY gained. At 6-month costs were lower and utilities were higher in outpatient, overpowering the inpatient procedure. Probabilistic sensitivity analysis showed that in 65% to 73% of simulations outpatient was the better option. The savings with outpatient were about 55% of inpatient values, with similar utility scores. No 30-day readmissions were recorded in either group.
Conclusion: This is the first economic study on cost-effectiveness of outpatient lumbar microdiscectomy, showing a significant reduction in costs, with a similar clinical outcome, proving it cost-effective.
Keywords: Cost–Benefit Analysis; Diskectomy; Economics; Intervertebral Disc Displacement; Outpatients; Patient Reported Outcome Measures.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures




References
LinkOut - more resources
Full Text Sources
Other Literature Sources
