

COMPARISON OF THE EFFECT OF THREE DIFFERENT DIETARY MODIFICATIONS ON MYOCARDIAL SUPPRESSION IN 18F-FDG PET/CT EVALUATION OF PATIENTS FOR SUSPECTED CARDIAC SARCOIDOSIS
- PMID: 33771904
- PMCID: PMC8612186
- DOI: 10.2967/jnumed.121.261981
COMPARISON OF THE EFFECT OF THREE DIFFERENT DIETARY MODIFICATIONS ON MYOCARDIAL SUPPRESSION IN 18F-FDG PET/CT EVALUATION OF PATIENTS FOR SUSPECTED CARDIAC SARCOIDOSIS
Abstract
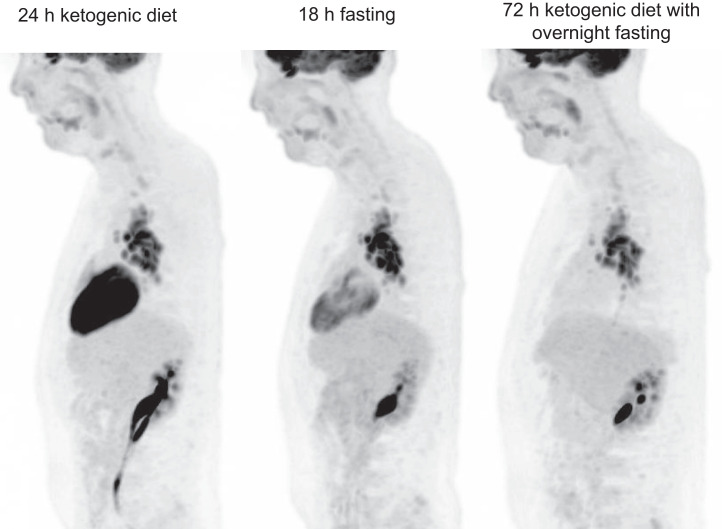
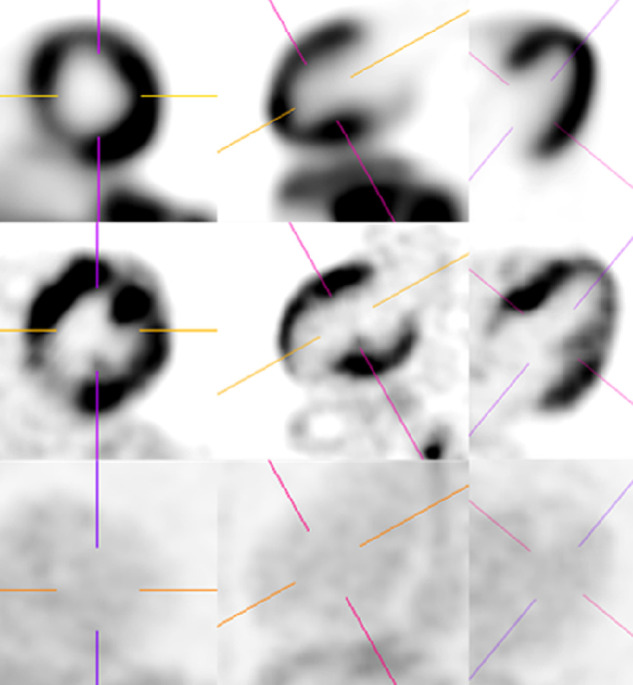
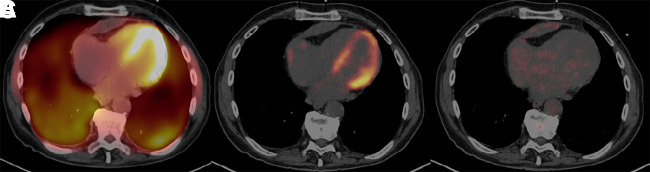
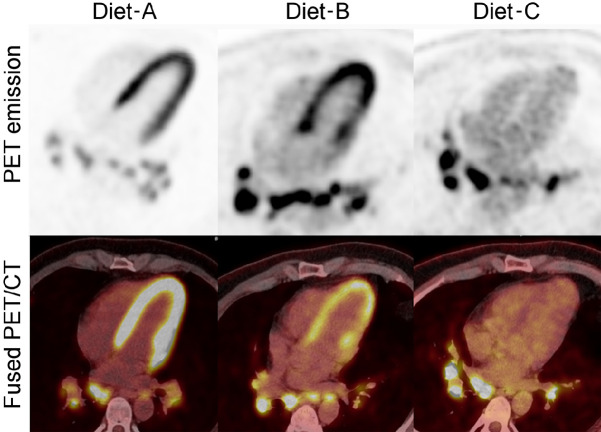
Rationale: A definitive dietary preparation recommendation is not possible based on literature in achievement of myocardial suppression for diagnosis of cardiac sarcoidosis (CS) with 18F-FDG PET/CT. Our goal is to compare three different dietary preparations in achievement of the best myocardial suppression and CS diagnosis. Methods: We retrospectively reviewed and compared three dietary preparations used at our institution. Three different diets were applied from 03/2014 to 12/2019. 24-h ketogenic diet with overnight fasting (n = 94); 18h-fasting (n = 44); 72-h daytime ketogenic diet with 3-day overnight fasting (n = 98). The interpretation of initial reports was recorded, and an independent radiologist (observer) retrospectively re-evaluated each case regarding CS diagnosis (Negative, Positive, Indeterminant) and myocardial suppression (Complete, Failed, Partial). Interobserver agreement was analyzed. We measured MaxSUV from bloodpool, liver, and the most suppressed normal myocardium. Results: We identified superior myocardial suppression with the 72-h preparation indicated by a higher bloodpool/myocardium and liver/myocardium ratios (P<0.001). Myocardial suppression rates for 72-h ketogenic diet, 24-h ketogenic diet and 18-h fasting preparations are as follows; Complete myocardial suppression: 96.9%/68.1%/52.3%, Failed myocardial suppression: 0%/23.4%/25%, Partial myocardial suppression: 3.1%/8.5%/22.7%) (P<0.001). The 72-hour preparation had significantly fewer "indeterminant" and "positive" exams. CS diagnosis rates for 72-h ketogenic diet, 24-h ketogenic diet and 18-h fasting preparations are as follows; Negative: 82.7%/52.1%/27.3%, Indeterminant: 2.0%/24.5%/40.9%, Positive: 15.3%/23.4%/31.8% (P<0.001). High agreement was present with the observer and the report (κ=0.88) Conclusion: A 72-h daytime ketogenic diet with 3-day overnight fasting, achieved substantially superior myocardial suppression versus 24-h ketogenic diet with overnight fasting and 18h-fasting using 18F-FDG PET/CT. This 72-h preparation results in significantly fewer "indeterminant" and potentially "false positive" CS results.
Keywords: Cardiac sarcoidosis; Cardiology (basic/technical); Cardiology (clinical); Fasting; Ketogenic diet; Myocardial suppression; PET/CT.
Copyright © 2021 by the Society of Nuclear Medicine and Molecular Imaging, Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources