

Compound heterozygous mutations in TGFBI cause a severe phenotype of granular corneal dystrophy type 2
- PMID: 33772078
- PMCID: PMC7997986
- DOI: 10.1038/s41598-021-86414-9
Compound heterozygous mutations in TGFBI cause a severe phenotype of granular corneal dystrophy type 2
Abstract
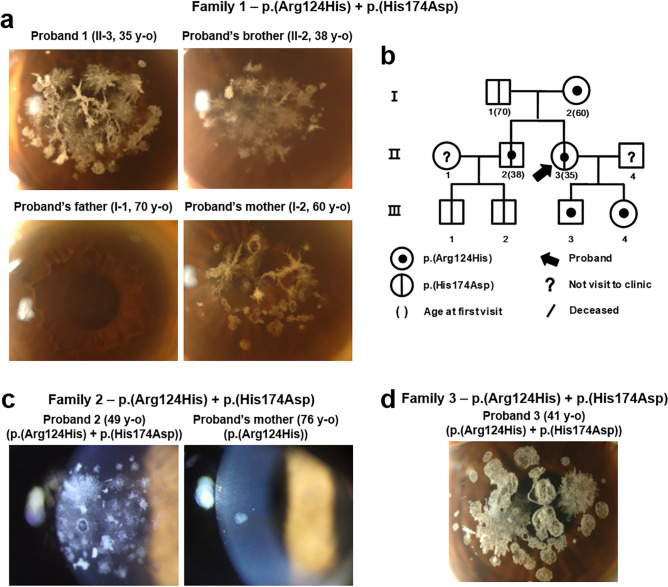
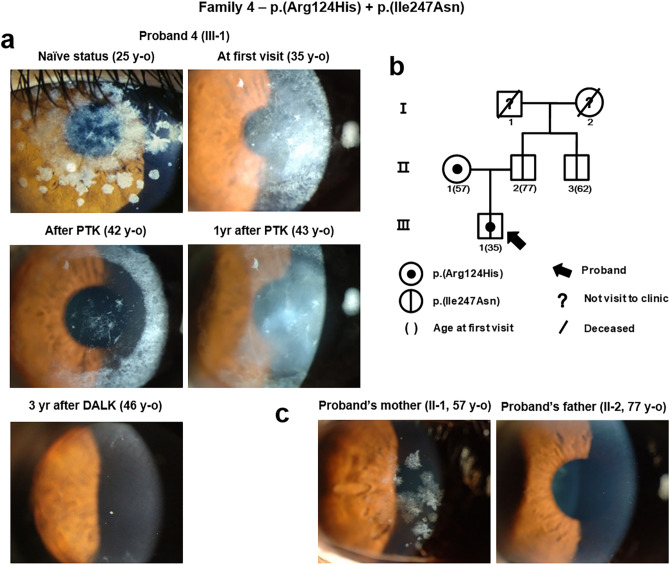
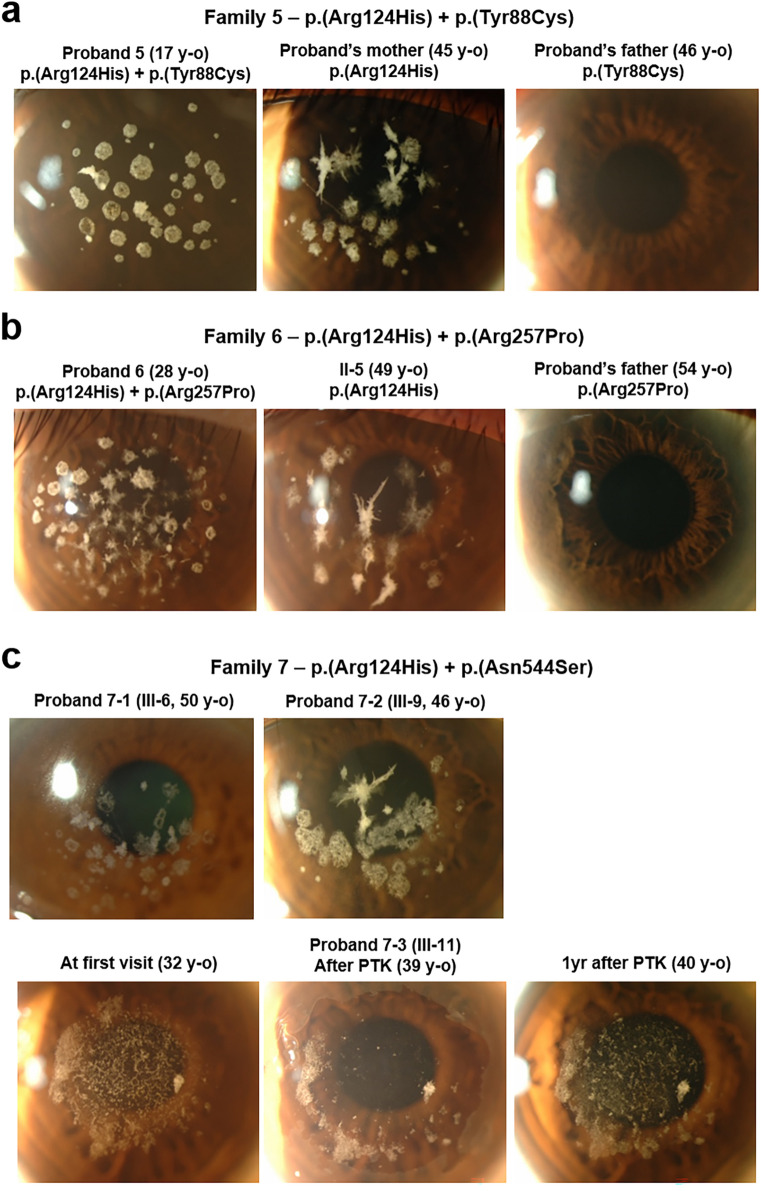
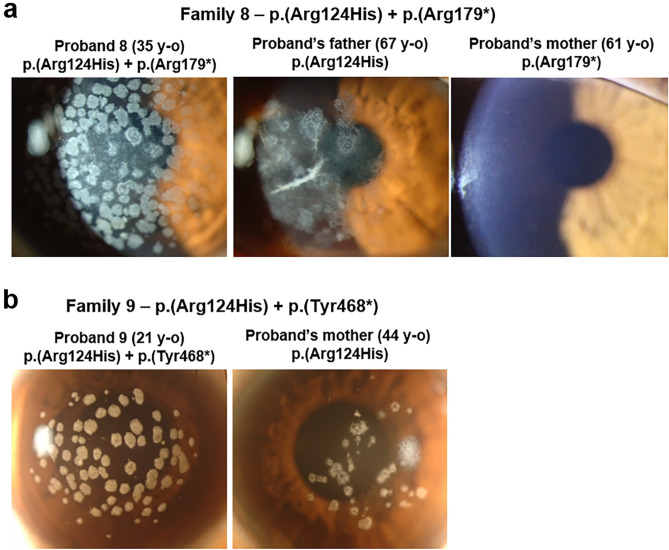
We investigated the clinical and genetic features of patients with severe phenotype of granular corneal dystrophy type 2 (GCD2) associated with compound heterozygosity in the transforming growth factor-β-induced (TGFBI) gene. Patients with severe GCD2 underwent ophthalmic examination (best-corrected visual acuity test, intraocular pressure measurement, slit-lamp examination, and slit-lamp photograph analysis) and direct Sanger sequencing of whole-TGFBI. The patient's family was tested to determine the pedigrees. Five novel mutations (p.(His174Asp), p.(Ile247Asn), p.(Tyr88Cys), p.(Arg257Pro), and p.(Tyr468*)) and two known mutations (p.(Asn544Ser) and p.(Arg179*)) in TGFBI were identified, along with p.(Arg124His), in the patients. Trans-phase of TGFBI second mutations was confirmed by pedigree analysis. Multiple, extensive discoid granular, and increased linear deposits were observed in the probands carrying p.(Arg124His) and other nonsense mutations. Some patients who had undergone phototherapeutic keratectomy experienced rapid recurrence (p.(Ile247Asn) and p.(Asn544Ser)); however, the cornea was well-maintained in a patient who underwent deep anterior lamellar keratoplasty (p.(Ile247Asn)). Thus, compound heterozygosity of TGFBI is associated with the phenotypic variability of TGFBI corneal dystrophies, suggesting that identifying TGFBI second mutations may be vital in patients with extraordinarily severe phenotypes. Our findings indicate the necessity for a more precise observation of genotype-phenotype correlation and additional care when treating TGFBI corneal dystrophies.
Conflict of interest statement
EKK is a medical advisory board member of Avellino Lab, USA. All other authors declare no competing interests.
Figures
References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
