

Opioid use and social disadvantage in patients with chronic musculoskeletal pain
- PMID: 33773068
- PMCID: PMC8464618
- DOI: 10.1002/pmrj.12596
Opioid use and social disadvantage in patients with chronic musculoskeletal pain
Abstract
Background: Historically, marginalized patients were prescribed less opioid medication than affluent, white patients. However, because of persistent differential access to nonopioid pain treatments, this direction of disparity in opioid prescribing may have reversed.
Objective: To compare social disadvantage and health in patients with chronic pain who were managed with versus without chronic opioid therapy. It was hypothesized that patients routinely prescribed opioids would be more likely to live in socially disadvantaged communities and report worse health.
Design: Cross-sectional analysis of a retrospective cohort defined from medical records from 2000 to 2019.
Setting: Single tertiary safety net medical center.
Patients: Adult patients with chronic musculoskeletal pain who were managed longitudinally by a physiatric group practice from at least 2011 to 2015 (n = 1173), subgrouped by chronic (≥4 years) adherent opioid usage (n = 356) versus no chronic opioid usage (n = 817).
Intervention: Not applicable.
Main outcome measures: The primary outcome was the unadjusted between-group difference in social disadvantage, defined by living in the worst national quartile of the Area Deprivation Index (ADI). An adjusted effect size was also calculated using logistic regression, with age, sex, race, and Patient-Reported Outcomes Measurement Information System (PROMIS) Pain Interference and Physical Function scores as covariates. Secondary outcomes included adjusted differences in health by chronic opioid use (measured by PROMIS).
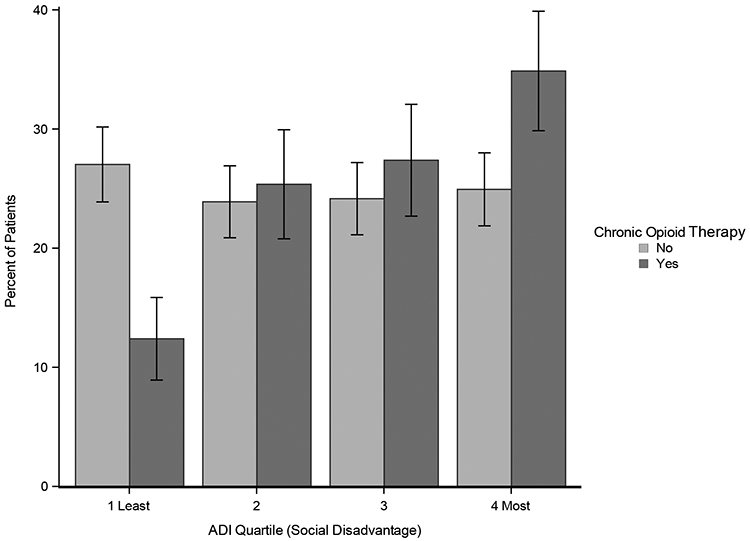
Results: Patients managed with chronic opioid therapy were more likely to live in a zip code within the most socially disadvantaged national quartile (34.9%; 95% confidence interval [CI] 29.9-39.9%; vs. 24.9%; 95% CI 21.9-28.0%; P < .001), and social disadvantage was independently associated with chronic opioid use (odds ratio [OR] 1.01 per ADI percentile [1.01-1.02]). Opioid use was also associated with meaningfully worse PROMIS Depression (3.8 points [2.4-5.1]), Anxiety (3.0 [1.4-4.5]), and Pain Interference (2.6 [1.7-3.5]) scores.
Conclusions: Patients prescribed chronic opioid treatment were more likely to live in socially disadvantaged neighborhoods, and chronic opioid use was independently associated with worse behavioral health. Improving access to multidisciplinary, nonopioid treatments for chronic pain may be key to successfully overcoming the opioid crisis.
© 2021 American Academy of Physical Medicine and Rehabilitation.
Figures

Similar articles
-
What is the Impact of Social Deprivation on Physical and Mental Health in Orthopaedic Patients?Clin Orthop Relat Res. 2019 Aug;477(8):1825-1835. doi: 10.1097/CORR.0000000000000698. Clin Orthop Relat Res. 2019. PMID: 31107333 Free PMC article.
-
Is Social Deprivation Associated with PROMIS Outcomes After Upper Extremity Fractures in Children?Clin Orthop Relat Res. 2021 Apr 1;479(4):826-834. doi: 10.1097/CORR.0000000000001571. Clin Orthop Relat Res. 2021. PMID: 33196588 Free PMC article.
-
Trends in opioid prescribing and co-prescribing of sedative hypnotics for acute and chronic musculoskeletal pain: 2001-2010.Pharmacoepidemiol Drug Saf. 2015 Aug;24(8):885-92. doi: 10.1002/pds.3776. Epub 2015 Apr 22. Pharmacoepidemiol Drug Saf. 2015. PMID: 25906971
-
Impact of COVID-19 pandemic on chronic pain and opioid use in marginalized populations: A scoping review.Front Public Health. 2023 Apr 17;11:1046683. doi: 10.3389/fpubh.2023.1046683. eCollection 2023. Front Public Health. 2023. PMID: 37139395 Free PMC article.
-
Opioids for chronic musculoskeletal pain: putting patient safety first.Pain. 2013 Dec;154(12):2583-2585. doi: 10.1016/j.pain.2013.09.017. Epub 2013 Sep 27. Pain. 2013. PMID: 24076163 Free PMC article. Review. No abstract available.
Cited by
-
Association of neighborhood-level disadvantage beyond individual sociodemographic factors in patients with or at risk of knee osteoarthritis.BMC Musculoskelet Disord. 2024 Nov 7;25(1):887. doi: 10.1186/s12891-024-08007-7. BMC Musculoskelet Disord. 2024. PMID: 39511529 Free PMC article.
-
Social support and the association between post-traumatic stress disorder and risk for long-term prescription opioid use.Pain. 2024 Oct 1;165(10):2379-2386. doi: 10.1097/j.pain.0000000000003286. Epub 2024 Jun 4. Pain. 2024. PMID: 38833573
-
Income-Based Disparities in Opioid Prescription Dispensing Among Public Drug Plan Beneficiaries in Canada from 2010 to 2018: A Population-Based and Sex-Stratified Retrospective Study.Drugs Real World Outcomes. 2025 Sep;12(3):337-349. doi: 10.1007/s40801-025-00498-7. Epub 2025 May 30. Drugs Real World Outcomes. 2025. PMID: 40445549 Free PMC article.
-
Patient understanding regarding opioid use in an orthopaedic trauma surgery population: a survey study.J Orthop Surg Res. 2021 Dec 24;16(1):736. doi: 10.1186/s13018-021-02881-w. J Orthop Surg Res. 2021. PMID: 34952626 Free PMC article.
-
Impacts of social determinants of health on chronic opioid therapy for chronic non-cancer pain.Pain Manag. 2024 Jun 2;14(5-6):251-257. doi: 10.1080/17581869.2024.2366145. Epub 2024 Jun 21. Pain Manag. 2024. PMID: 38904289 Free PMC article.
References
-
- Phillips DM. JCAHO pain management standards are unveiled. Joint Commission on Accreditation of Healthcare Organizations. JAMA. 2000;284(4):428–429. - PubMed
-
- Liu Y, Logan JE, Paulozzi LJ, Zhang K, Jones CM. Potential misuse and inappropriate prescription practices involving opioid analgesics. The American journal of managed care. 2013;19(8):648–658. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
