

Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD-based protein subunit vaccine (ZF2001) against COVID-19 in adults: two randomised, double-blind, placebo-controlled, phase 1 and 2 trials
- PMID: 33773111
- PMCID: PMC7990482
- DOI: 10.1016/S1473-3099(21)00127-4
Safety and immunogenicity of a recombinant tandem-repeat dimeric RBD-based protein subunit vaccine (ZF2001) against COVID-19 in adults: two randomised, double-blind, placebo-controlled, phase 1 and 2 trials
Abstract
Background: Although several COVID-19 vaccines have been developed so far, they will not be sufficient to meet the global demand. Development of a wider range of vaccines, with different mechanisms of action, could help control the spread of SARS-CoV-2 globally. We developed a protein subunit vaccine against COVID-19 using a dimeric form of the receptor-binding domain (RBD) of the SARS-CoV-2 spike protein as the antigen. We aimed to assess the safety and immunogenicity of this vaccine, ZF2001, and determine the appropriate dose and schedule for an efficacy study.
Methods: We did two randomised, double-blind, placebo-controlled, phase 1 and phase 2 trials. Phase 1 was done at two university hospitals in Chongqing and Beijing, China, and phase 2 was done at the Hunan Provincial Center for Disease Control and Prevention in Xiangtan, China. Healthy adults aged 18-59 years, without a history of SARS-CoV or SARS-CoV-2 infection, an RT-PCR-positive test result for SARS-CoV-2, a history of contact with confirmed or suspected COVID-19 cases, and severe allergies to any component of the vaccine were eligible for enrolment. In phase 1, participants were randomly assigned (2:2:1) to receive three doses of the vaccine (25 μg or 50 μg) or placebo intramuscularly, 30 days apart. In phase 2, participants were randomly assigned (1:1:1:1:1:1) to receive the vaccine (25 μg or 50 μg) or placebo intramuscularly, 30 days apart, in either a two-dose schedule or a three-dose schedule. Investigators, participants, and the laboratory team were masked to group allocation. For phase 1, the primary outcome was safety, measured by the occurrence of adverse events and serious adverse events. For phase 2, the primary outcome was safety and immunogenicity (the seroconversion rate and the magnitude, in geometric mean titres [GMTs], of SARS-CoV-2-neutralising antibodies). Analyses were done on an intention-to-treat and per-protocol basis. These trials are registered with ClinicalTrials.gov (NCT04445194 and NCT04466085) and participant follow-up is ongoing.
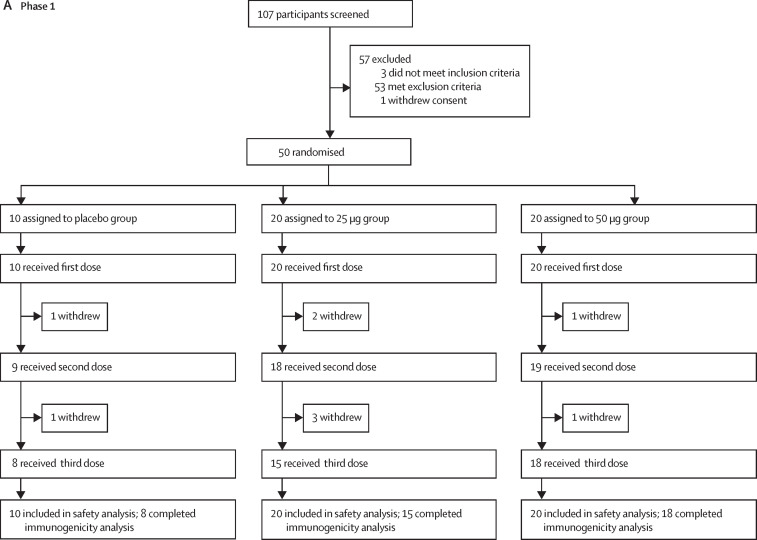
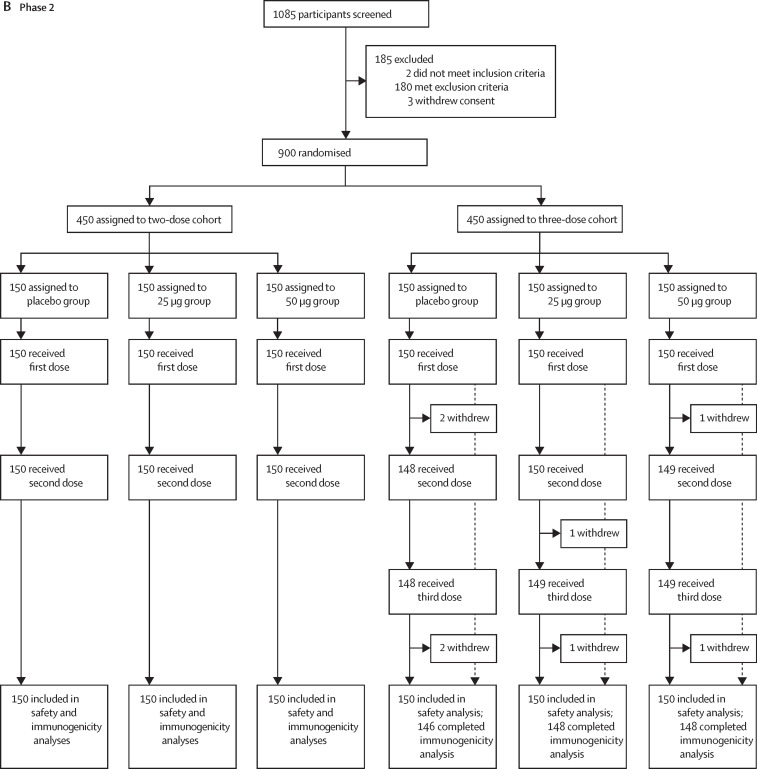
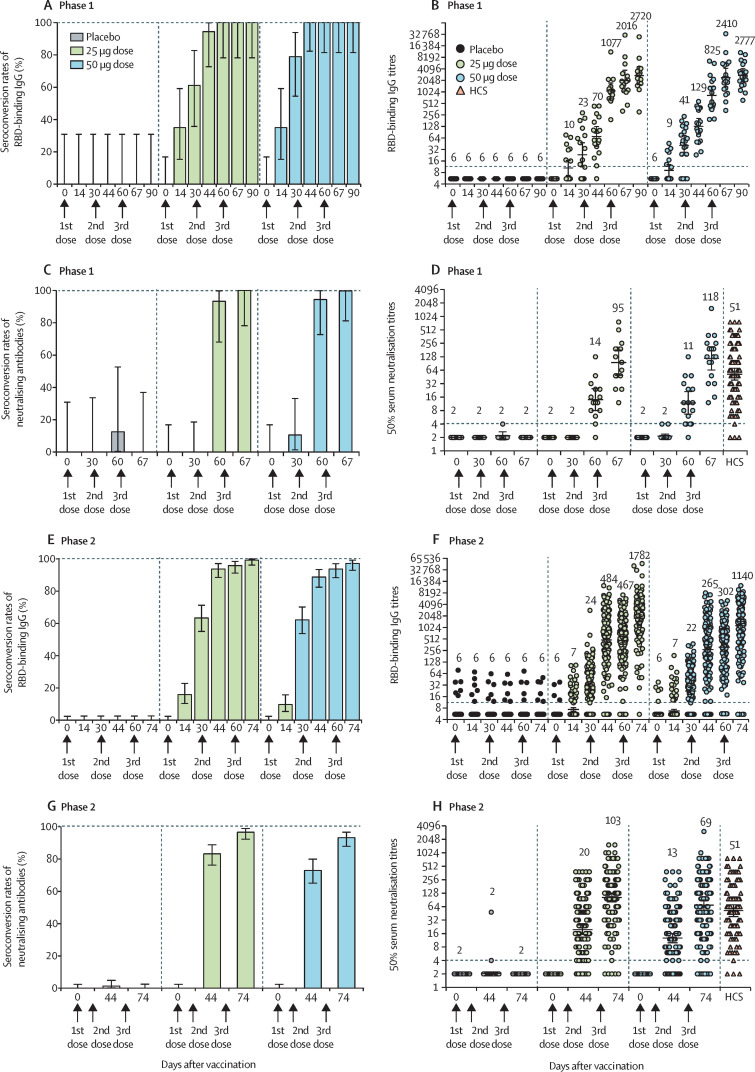
Findings: Between June 22 and July 3, 2020, 50 participants were enrolled into the phase 1 trial and randomly assigned to receive three doses of placebo (n=10), the 25 μg vaccine (n=20), or the 50 μg vaccine (n=20). The mean age of participants was 32·6 (SD 9·4) years. Between July 12 and July 17, 2020, 900 participants were enrolled into the phase 2 trial and randomly assigned to receive two doses of placebo (n=150), 25 μg vaccine (n=150), or 50 μg vaccine (n=150), or three doses of placebo (n=150), 25 μg vaccine (n=150), or 50 μg vaccine (n=150). The mean age of participants was 43·5 (SD 9·2) years. In both phase 1 and phase 2, adverse events reported within 30 days after vaccination were mild or moderate (grade 1 or 2) in most cases (phase 1: six [60%] of ten participants in the placebo group, 14 [70%] of 20 in the 25 μg group, and 18 [90%] of 20 in the 50 μg group; phase 2: 37 [25%] of 150 in the two-dose placebo group, 43 [29%] of 150 in the two-dose 25 μg group, 50 [33%] of 150 in the two-dose 50 μg group, 47 [31%] of 150 in the three-dose placebo group, 72 [48%] of 150 in the three-dose 25 μg group, and 65 [43%] of 150 in the three-dose 50 μg group). In phase 1, two (10%) grade 3 or worse adverse events were reported in the 50 μg group. In phase 2, grade 3 or worse adverse events were reported by 18 participants (four [3%] in the two-dose 25 μg vaccine group, two [1%] in the two-dose 50 μg vaccine group, two [1%] in the three-dose placebo group, four [3%] in the three-dose 25 μg vaccine group, and six [4%] in the three-dose 50 μg vaccine group), and 11 were considered vaccine related (two [1%] in the two-dose 25 μg vaccine group, one [1%] in the two-dose 50 μg vaccine group, one [1%] in the three-dose placebo group, two [1%] in the three-dose 25 μg vaccine group, and five [3%] in the three-dose 50 μg vaccine group); seven participants reported serious adverse events (one [1%] in the two-dose 25 μg vaccine group, one [1%] in the two-dose 50 μg vaccine group, two [1%] in the three-dose placebo group, one [1%] in the three-dose 25 μg vaccine group, and two [1%] in the three-dose 50 μg vaccine group), but none was considered vaccine related. In phase 2, on the two-dose schedule, seroconversion rates of neutralising antibodies 14 days after the second dose were 76% (114 of 150 participants) in the 25 μg group and 72% (108 of 150) in the 50 μg group; on the three-dose schedule, seroconversion rates of neutralising antibodies 14 days after the third dose were 97% (143 of 148 participants) in the 25 μg group and 93% (138 of 148) in the 50 μg group. In the two-dose groups in phase 2, the SARS-CoV-2-neutralising GMTs 14 days after the second dose were 17·7 (95% CI 13·6-23·1) in the 25 μg group and 14·1 (10·8-18·3) in the 50 μg group. In the three-dose groups in phase 2, the SARS-CoV-2-neutralising GMTs 14 days after the third dose were 102·5 (95% CI 81·8-128·5) in the 25 μg group and 69·1 (53·0-90·0) in the 50 μg group.
Interpretation: The protein subunit vaccine ZF2001 appears to be well tolerated and immunogenic. The safety and immunogenicity data from the phase 1 and 2 trials support the use of the 25 μg dose in a three-dose schedule in an ongoing phase 3 trial for large-scale evaluation of ZF2001's safety and efficacy.
Funding: National Program on Key Research Project of China, National Science and Technology Major Projects of Drug Discovery, Strategic Priority Research Program of the Chinese Academy of Sciences, and Anhui Zhifei Longcom Biopharmaceutical.
Translation: For the Chinese translation of the abstract see Supplementary Materials section.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests YLi, LD, JY, and GFG are listed in the patent as the inventors of the RBD dimer as a betacoronavirus vaccine. All other authors declare no competing interests.
Figures
Comment in
-
Is there space for a three-dose vaccine to fight the spread of SARS-CoV-2?Lancet Infect Dis. 2021 Aug;21(8):1054-1055. doi: 10.1016/S1473-3099(21)00149-3. Epub 2021 Mar 24. Lancet Infect Dis. 2021. PMID: 33773112 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
