

Diagnostic and analytical performance evaluation of ten commercial assays for detecting SARS-CoV-2 humoral immune response
- PMID: 33773989
- PMCID: PMC7989098
- DOI: 10.1016/j.jim.2021.113043
Diagnostic and analytical performance evaluation of ten commercial assays for detecting SARS-CoV-2 humoral immune response
Abstract
Objective: Analytical validation of newly released SARS-CoV-2 antibody assays in the clinical laboratory is crucial to ensure sufficient performance in respect to its intended use. We aimed to assess analytical and diagnostic performance of 8 (semi-)quantitative assays detecting anti-nucleocapsid IgG (Euroimmun, Id-Vet) or total Ig (Roche), anti-spike protein IgG (Euroimmun, Theradiag, DiaSorin, Thermo Fisher) or both (Theradiag) and 2 rapid lateral flow assays (LFA) (AAZ-LMB and Theradiag).
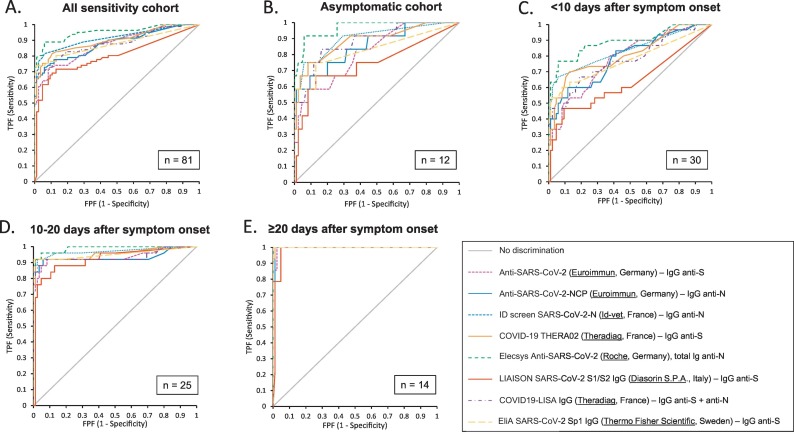
Methods: Specificity was evaluated using a cross-reactivity panel of 85 pre-pandemic serum samples. Sensitivity was determined at both the manufacturer's and a 95% specificity cut-off level, using 81 serum samples of patients with a positive rRT-PCR. Sensitivity was determined in function of time post symptoms onset.
Results: Specificity for all assays ranged from 92.9% to 100% (Roche and Thermo Fisher) with the exception of the Theradiag IgM LFA (82.4%). Sensitivity in asymptomatic patients ranged between 41.7% and 58.3%. Sensitivity on samples taken <10 days since symptom onset was low (23.3%-66.7%) and increased on samples taken between 10 and 20 days and > 20 days since symptom onset (80%-96% and 92.9%-100%, respectively). From 20 days after symptom onset, the Roche, Id-vet and Thermo Fisher assays all met the sensitivity (>95%) and specificity (>97%) targets determined by the WHO. Antibody signal response was significantly higher in the critically ill patient group.
Conclusion: Antibody detection can complement rRT-PCR for the diagnosis of COVID-19, especially in the later stage, or in asymptomatic patients for epidemiological purposes. Addition of IgM in LFAs did not improve sensitivity.
Keywords: Antibody; COVID-19; Humoral response; SARS-CoV-2; Serology.
Copyright © 2021 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
AB and LVH have been consultants for Thermo Fisher Scientific.
Figures
References
-
- Bohn M.K., Lippi G., Horvath A., Sethi S., Koch D., Ferrari M., et al. Molecular, serological, and biochemical diagnosis and monitoring of COVID-19: IFCC taskforce evaluation of the latest evidence. Clin. Chem. Lab. Med. 2020 Jun;58(7):1037–1052. - PubMed
-
- Burbelo P.D., Riedo F.X., Morishima C., Rawlings S., Smith D., Das S., et al. Sensitivity in detection of antibodies to Nucleocapsid and spike proteins of severe acute respiratory syndrome coronavirus 2 in patients with coronavirus disease 2019. J. Infect. Dis. 2020 Jun;222(2):206–213. - PMC - PubMed
-
- Centers for Disease Control and Prevention . 2020. Interim Guidelines for Collecting, Handling, and Testing Clinical Specimens from Persons for Coronavirus Disease 2019 (COVID-19)
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
