

The accuracy of coronary CT angiography in patients with coronary calcium score above 1000 Agatston Units: Comparison with quantitative coronary angiography
- PMID: 33775584
- PMCID: PMC8403134
- DOI: 10.1016/j.jcct.2021.03.007
The accuracy of coronary CT angiography in patients with coronary calcium score above 1000 Agatston Units: Comparison with quantitative coronary angiography
Abstract
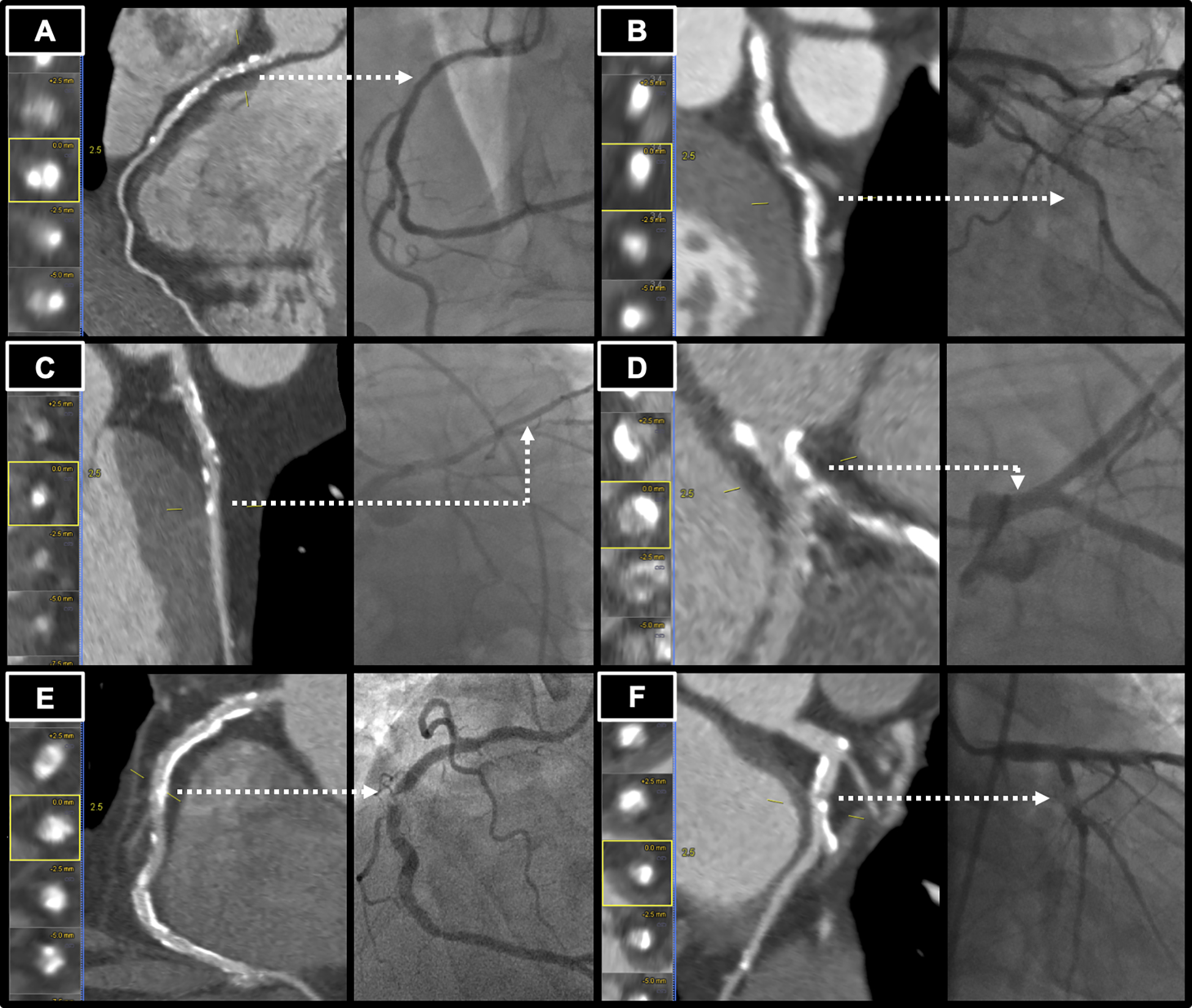
Background: High amounts of coronary artery calcium (CAC) pose challenges in interpretation of coronary CT angiography (CCTA). The accuracy of stenosis assessment by CCTA in patients with very extensive CAC is uncertain.
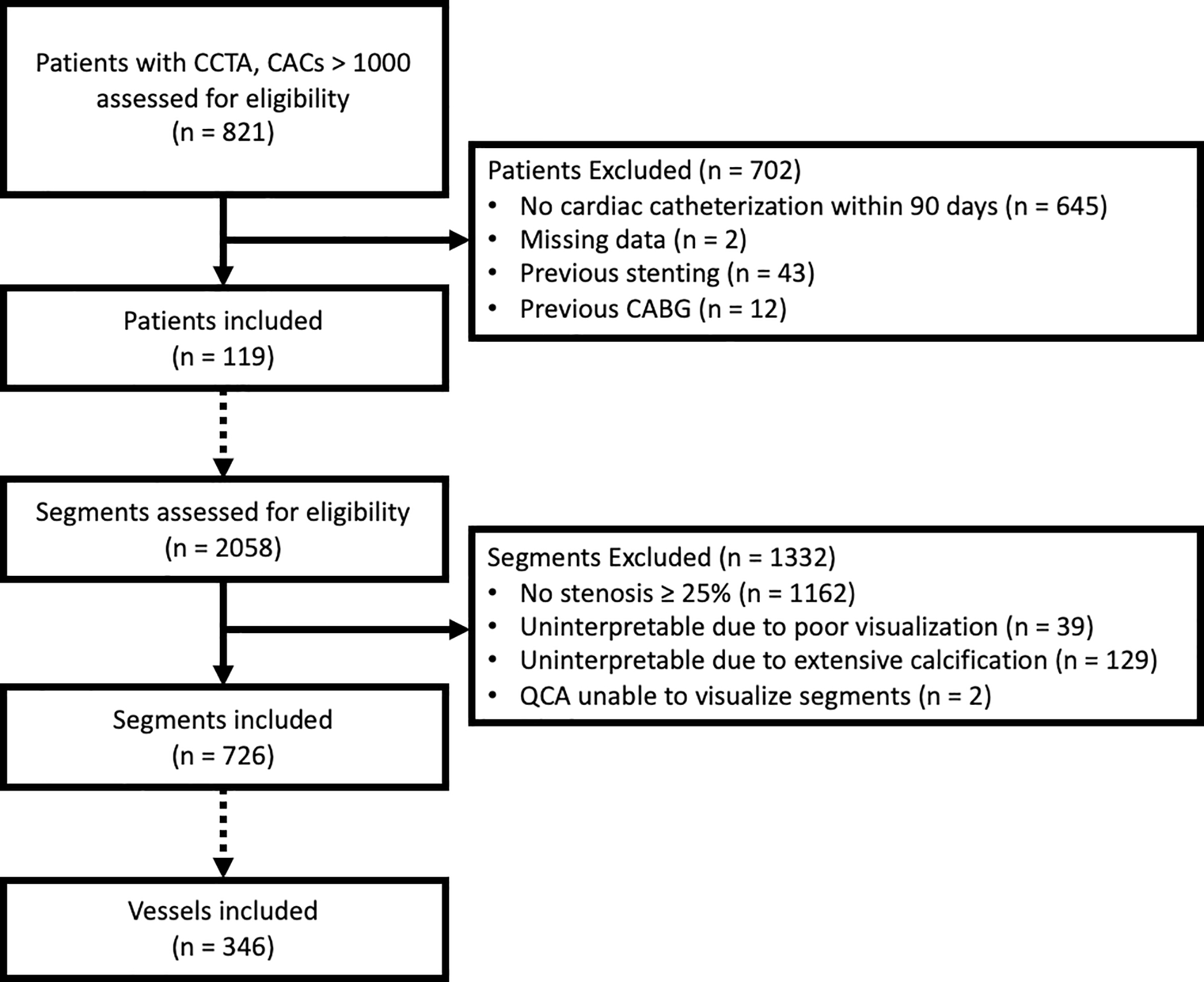
Methods: Retrospective study was performed including patients who underwent clinically directed CCTA with CAC score >1000 and invasive coronary angiography within 90 days. Segmental stenosis on CCTA was graded by visual inspection with two-observer consensus using categories of 0%, 1-24%, 25-49%, 50-69%, 70-99%, 100% stenosis, or uninterpretable. Blinded quantitative coronary angiography (QCA) was performed on all segments with stenosis ≥25% by CCTA. The primary outcome was vessel-based agreement between CCTA and QCA, using significant stenosis defined by diameter stenosis ≥70%. Secondary analyses on a per-patient basis and inclusive of uninterpretable segments were performed.
Results: 726 segments with stenosis ≥25% in 346 vessels within 119 patients were analyzed. Median coronary calcium score was 1616 (1221-2118). CCTA identification of QCA-based stenosis resulted in a per-vessel sensitivity of 79%, specificity of 75%, positive predictive value (PPV) of 45%, negative predictive value (NPV) of 93%, and accuracy 76% (68 false positive and 15 false negative). Per-patient analysis had sensitivity 94%, specificity 55%, PPV 63%, NPV 92%, and accuracy 72% (30 false-positive and 3 false-negative). Inclusion of uninterpretable segments had variable effect on sensitivity and specificity, depending on whether they are considered as significant or non-significant stenosis.
Conclusions: In patients with very extensive CAC (>1000 Agatston units), CCTA retained a negative predictive value > 90% to identify lack of significant stenosis on a per-vessel and per-patient level, but frequently overestimated stenosis.
Keywords: Accuracy; Coronary CT angiography; Coronary artery calcium; Coronary calcium score; Quantitative coronary angiography; Stenosis.
Copyright © 2021 Society of Cardiovascular Computed Tomography. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors report no conflicts of interest.
Figures
References
-
- Kalisz K, Buethe J, Saboo SS, Abbara S, Halliburton S, Rajiah P. Artifacts at cardiac CT: physics and solutions. Radiographics. 2016;36:2064–2083. - PubMed
-
- Cheng V, Gutstein A, Wolak A, et al.Moving beyond binary grading of coronary arterial stenoses on coronary computed tomographic angiography: insights for the imager and referring clinician. JACC: Cardiovascular Imaging. 2008;1:460–471. - PubMed
-
- Ong TK, Chin SP, Liew CK, et al.Accuracy of 64-row multidetector computed tomography in detecting coronary artery disease in 134 symptomatic patients: influence of calcification. American heart journal. 2006;151:1323. e1321–1323. e1326. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
