

Chronic renal dysfunction in cirrhosis: A new frontier in hepatology
- PMID: 33776368
- PMCID: PMC7985728
- DOI: 10.3748/wjg.v27.i11.990
Chronic renal dysfunction in cirrhosis: A new frontier in hepatology
Abstract
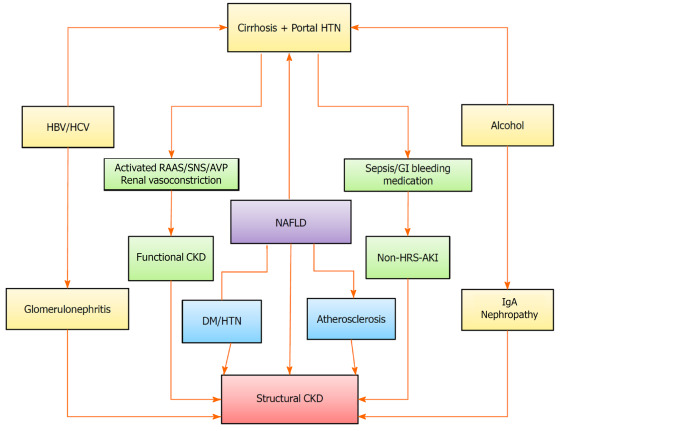
Chronic kidney disease (CKD) in patients with liver cirrhosis has become a new frontier in hepatology. In recent years, a sharp increase in the diagnosis of CKD has been observed among patients with cirrhosis. The rising prevalence of risk factors, such as diabetes, hypertension and nonalcoholic fatty liver disease, appears to have contributed significantly to the high prevalence of CKD. Moreover, the diagnosis of CKD in cirrhosis is now based on a reduction in the estimated glomerular filtration rate of < 60 mL/min over more than 3 mo. This definition has resulted in a better differentiation of CKD from acute kidney injury (AKI), leading to its greater recognition. It has also been noted that a significant proportion of AKI transforms into CKD in patients with decompensated cirrhosis. CKD in cirrhosis can be structural CKD due to kidney injury or functional CKD secondary to circulatory and neurohormonal imbalances. The available literature on combined cirrhosis-CKD is extremely limited, as most attempts to assess renal dysfunction in cirrhosis have so far concentrated on AKI. Due to problems related to glomerular filtration rate estimation in cirrhosis, the absence of reliable biomarkers of CKD and technical difficulties in performing renal biopsy in advanced cirrhosis, CKD in cirrhosis can present many challenges for clinicians. With combined hepatorenal dysfunctions, fluid mobilization becomes problematic, and there may be difficulties with drug tolerance, hemodialysis and decision-making regarding the need for liver vs simultaneous liver and kidney transplantation. This paper offers a thorough overview of the increasingly known CKD in patients with cirrhosis, with clinical consequences and difficulties occurring in the diagnosis and treatment of such patients.
Keywords: Acute kidney injury; Chronic kidney disease; Cirrhosis; Hepatorenal syndrome; Renal failure; Renal function.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest for this article.
Figures
References
-
- Péron JM, Bureau C, Gonzalez L, Garcia-Ricard F, de Soyres O, Dupuis E, Alric L, Pourrat J, Vinel JP. Treatment of hepatorenal syndrome as defined by the international ascites club by albumin and furosemide infusion according to the central venous pressure: a prospective pilot study. Am J Gastroenterol. 2005;100:2702–2707. - PubMed
-
- Solà E, Ginès P. Chronic Kidney Disease in Cirrhosis: Emerging Complication With Negative Impact in the Liver Transplant Setting. Liver Transpl. 2020;26:483–484. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
