

The Good Treatment, the Bad Virus, and the Ugly Inflammation: Pathophysiology of Kidney Involvement During COVID-19
- PMID: 33776785
- PMCID: PMC7993058
- DOI: 10.3389/fphys.2021.613019
The Good Treatment, the Bad Virus, and the Ugly Inflammation: Pathophysiology of Kidney Involvement During COVID-19
Abstract
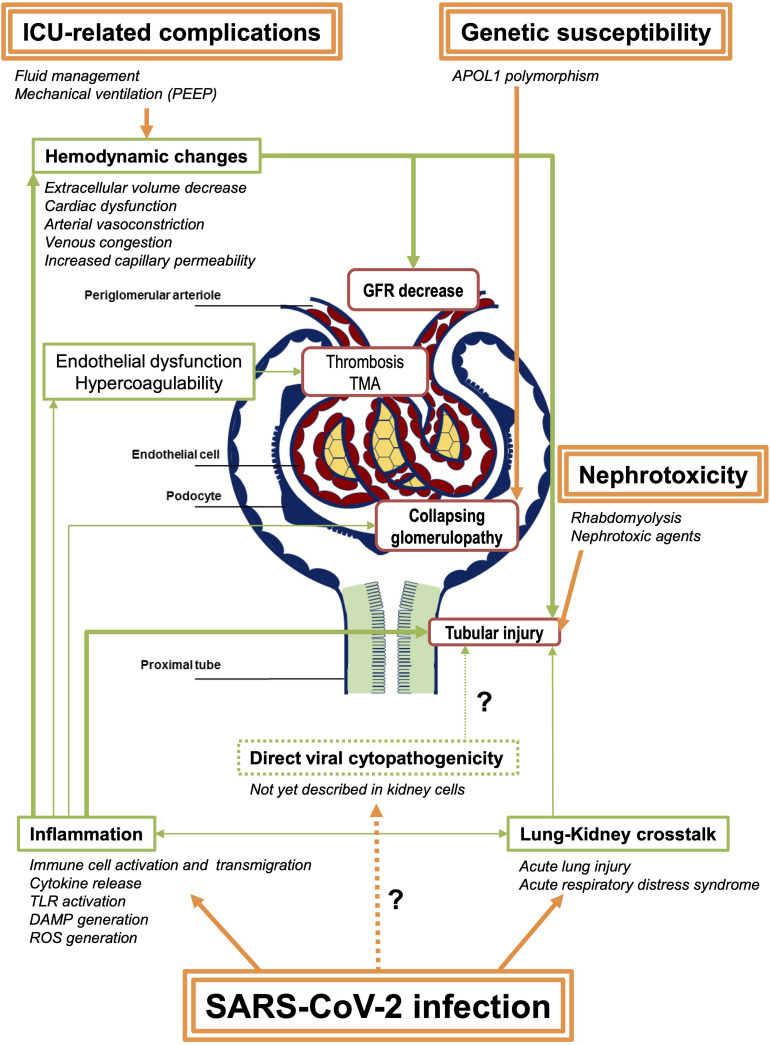
Kidney involvement is a common complication during SARS-CoV-2 infection. Its association with poor outcomes, especially in critically ill patients, raises issues whether kidney involvement reflects multi-organ damage or if it is a specific feature of the infection. Based on observational studies, autopsy series, and on current understanding of the route of entry of the virus, this review will highlight the different types of kidney involvement during COVID-19 and put them in the perspective of the different pathophysiological hypotheses. Virus entry route through ACE2 ligation and TMPRSS2 coligation allows identifying potential viral targets in the kidney, including tubules, endothelial cells, and glomerulus. While reports have described damages of all these structures and virus kidney tropism has been identified in renal extracts in autopsy series, no direct viral infection has been found in the latter structures thus far on kidney biopsies. Notwithstanding the technical challenge of disclosing viral invasion within tissues and cells, viral direct cytopathogenic effect generally does not appear as the cause of the observed renal damage. Inflammation and altered hemodynamics, described as "viral sepsis," might rather be responsible for organ dysfunction, including kidneys. We shall place these various mechanisms into an integrated vision where the synergy between direct viral pathogenicity and systemic inflammation enhances renal damage. As SARS-CoV-2 inexorably continues its rampant spread, understanding the sequence of events in the kidneys might thus help inform improved therapeutic strategies, including antiviral drugs and immunomodulators.
Keywords: AKI (acute kidney injury); COVID; COVID–19; SARS – CoV – 2; inflammation; kidney; viral sepsis.
Copyright © 2021 Le Stang, Desenclos, Flamant, Chousterman and Tabibzadeh.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Akilesh S., Nast C. C., Yamashita M., Henriksen K., Charu V., Troxell M. L., et al. (2020). Multicenter clinicopathologic correlation of kidney biopsies performed in COVID-19 patients presenting with acute kidney injury or proteinuria. Am. J. Kidney Dis. 77 82.e–93.e. 10.1053/j.ajkd.2020.10.001 - DOI - PMC - PubMed
-
- Arrestier R., Stehle T., Letavernier E., Mekontso-Dessap A. (2020). Lopinavir-ritonavir associated acute kidney injury is not related to crystalluria in critically-ill COVID-19 patients. Lopinavir-ritonavir associated acute kidney injury is not related to crystalluria in critically-ill COVID-19 patients. Kidney Int. Rep. 5:2119. 10.1016/j.ekir.2020.08.021 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous