

The Burden of Antipsychotic-Induced Weight Gain and Metabolic Syndrome in Children
- PMID: 33776816
- PMCID: PMC7994286
- DOI: 10.3389/fpsyt.2021.623681
The Burden of Antipsychotic-Induced Weight Gain and Metabolic Syndrome in Children
Abstract
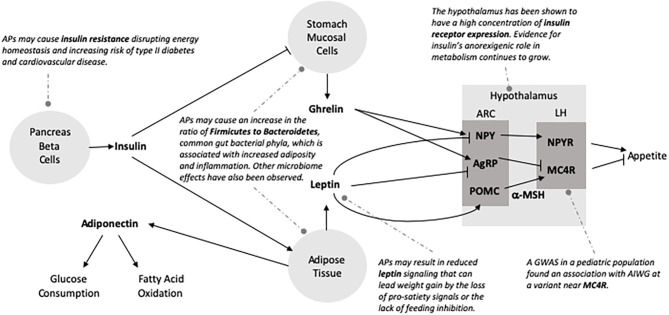
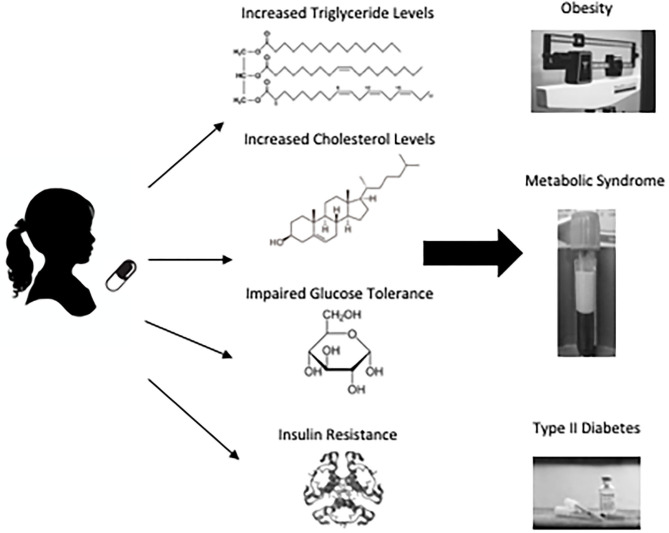
Antipsychotic medications are critical to child and adolescent psychiatry, from the stabilization of psychotic disorders like schizophrenia, bipolar disorder, and psychotic depression to behavioral treatment of autism spectrum disorder, tic disorders, and pediatric aggression. While effective, these medications carry serious risk of adverse events-most commonly, weight gain and cardiometabolic abnormalities. Negative metabolic consequences affect up to 60% of patients and present a major obstacle to long-term treatment. Since antipsychotics are often chronically prescribed beginning in childhood, cardiometabolic risk accumulates. An increased susceptibility to antipsychotic-induced weight gain (AIWG) has been repeatedly documented in children, particularly rapid weight gain. Associated cardiometabolic abnormalities include central obesity, insulin resistance, dyslipidemia, and systemic inflammation. Lifestyle interventions and medications such as metformin have been proposed to reduce risk but remain limited in efficacy. Furthermore, antipsychotic medications touted to be weight-neutral in adults can cause substantial weight gain in children. A better understanding of the biological underpinnings of AIWG could inform targeted and potentially more fruitful treatments; however, little is known about the underlying mechanism. As yet, modest genetic studies have nominated a few risk genes that explain only a small percentage of the risk. Recent investigations have begun to explore novel potential mechanisms of AIWG, including a role for gut microbiota and microbial metabolites. This article reviews the problem of AIWG and AP metabolic side effects in pediatric populations, proposed mechanisms underlying this serious side effect, and strategies to mitigate adverse impact. We suggest future directions for research efforts that may advance the field and lead to improved clinical interventions.
Keywords: adverse drug effects; antipsychotic-induced weight gain; antipsychotics; child psychiatry; metabolic syndrome; pediatrics.
Copyright © 2021 Libowitz and Nurmi.
Conflict of interest statement
EN serves on the Medical Advisory Board for the Tourette Association of America and Teva Pharmaceuticals and the Scientific Advisory Board for Myriad Genetics. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials