

Clinical and VNG Features in Anterior Canal BPPV-An Analysis of 13 Cases
- PMID: 33776883
- PMCID: PMC7988206
- DOI: 10.3389/fneur.2021.618269
Clinical and VNG Features in Anterior Canal BPPV-An Analysis of 13 Cases
Abstract
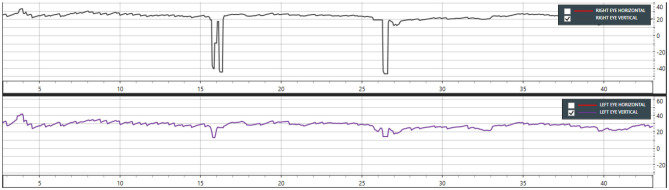
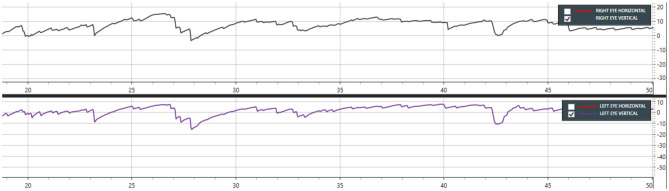
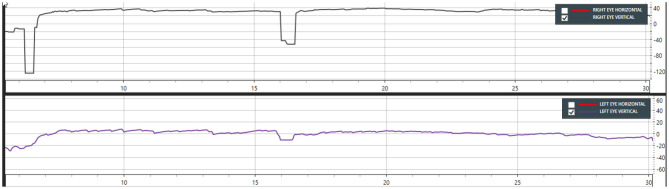
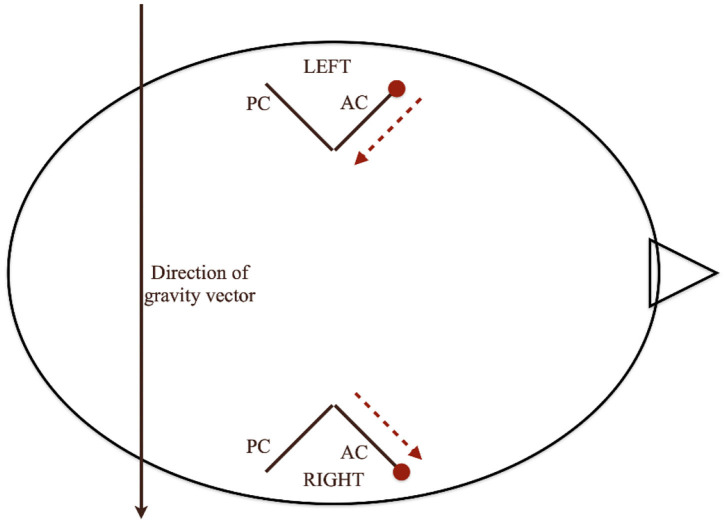
Objective: To define diagnostic VNG features in anterior canal BPPV during positional testing (Dix-Hallpike, supine head hanging, and McClure Pagnini tests). Study Design: A retrospective study of patients diagnosed with anterior canal BPPV across four referral centers in New Delhi, Kochi, Bangalore, and Dubai. Subjects and Methods: Clinical records of 13 patients with AC BPPV out of 1,350 cases, during a 3-years period, were reviewed and analyzed by four specialists. Results: Four patients had positional down beating nystagmus with symptoms of vertigo during the bilateral DHP maneuver. Seven cases had positional down beating nystagmus only on one side of DHP. Typical down beating nystagmus was seen in 10 out of 13 cases during the straight head hanging maneuver. Down beating torsional nystagmus was seen in 6 out of 13 cases. Down beating with horizontal nystagmus was seen in three cases (in DHP and MCP mainly) while pure down beating nystagmus during SHH was only seen in four cases. Conclusion: We conclude that anterior canal BPPV is a rare but definite entity. It may not be apparent on positional testing the first time, so repeated testing may be needed. The most consistent diagnostic maneuver is SHH though there were patients in which findings could only be elicited using DHP testing. We recommend a testing protocol that includes DHP testing on both sides and SHH. MCP testing may also evoke DBN with or without the torsional component. Reversal of nystagmus on reversal of testing position is unusual but can occur. The Yacovino maneuver is effective in resolving AC BPPV. We also propose a hypothesis that explains why DHP testing is sensitive to AC BPPV on either side, whereas MCP lateral position on one side is only sensitive to AC BPPV on one side. We have explained a possible role for the McClure Pagnini test in side determination and therapeutic implications.
Keywords: Anterior canal BPPV; Benign paroxysmal positional vertigo; Dix Hallpike test; Down beating Nystagmus; McClure Pagnini; VNG; VNG features; Yacovino maneuver.
Copyright © 2021 Porwal, V. R., Pawar, Dorasala, Bijlani, Nair and Nayar.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Honrubia V, Baloh RW, Harris MR, Jacobson KM. Paroxysmal positional vertigo syndrome. Am J Otol. (1999) 20:465–70. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous