

Evaluation of Immune and Vaccine Competence in Steroid-Sensitive Nephrotic Syndrome Pediatric Patients
- PMID: 33776994
- PMCID: PMC7994282
- DOI: 10.3389/fimmu.2021.602826
Evaluation of Immune and Vaccine Competence in Steroid-Sensitive Nephrotic Syndrome Pediatric Patients
Abstract
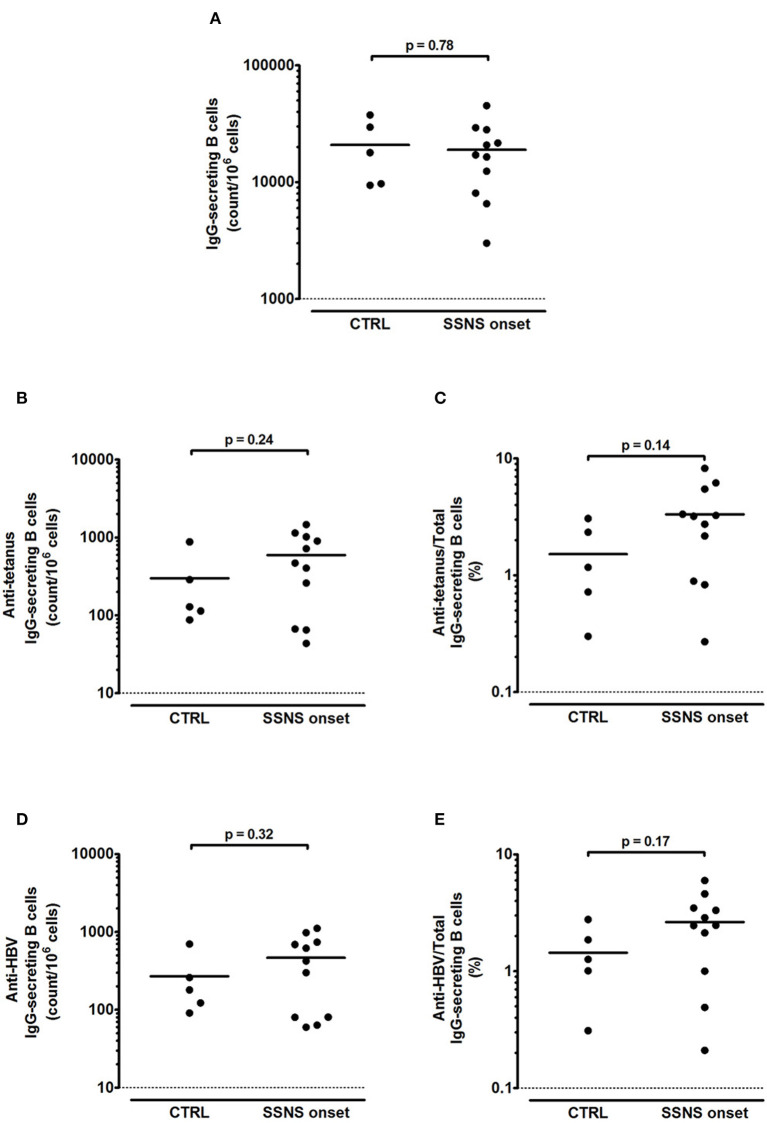
Idiopathic nephrotic syndrome is a childhood renal disease characterized by a damage of the glomerular filtration barrier leading to an intense leakage of proteins into the urine. This severe proteinuria causes a transient but strong reduction of serum IgG. Therefore, evaluation of vaccine competence by measuring serum levels of protective antibodies can be misleading in nephrotic syndrome, especially during the active phase of disease. To overcome this issue, in parallel to measuring serum antigen-specific IgG, we quantified by ELISPOT the number of antigen-specific memory B cells induced by previous immunization with tetanus and hepatitis B virus (HBV) in 11 steroid-sensitive nephrotic syndrome (SSNS) pediatric patients at onset before any immunosuppressive treatment (mean age 5.1±0.9 years). Five age-matched children with non-immunomediated nephro-urologic disorders were also enrolled as controls (mean age 6.9±2.3 years). Low total serum IgG levels (<520 mg/dl) were found in all the analyzed SSNS patients. In parallel, median levels of anti-tetanus and anti-HBV IgG were significantly reduced compared to controls [0.05 (0.03-0.16) vs. 0.45 (0.29-3.10) IU/ml and 0.0 (0.0-0.5) vs. 30.3 (5.5-400.8) mIU/ml, respectively; p = 0.02 for both], with serum IgG titers below protective threshold in 7/11 SSNS patients for tetanus and in 9/11 SSNS patients for HBV. In contrast, all SSNS patients had a competent B-cell response, showing an amount of total IgG-secreting B cells >1,000 counts/106 stimulated cells. The amount of anti-tetanus and anti-HBV IgG-secreting B cells was also comparable to that of controls (p = 0.24, p = 0.32, respectively), with a frequency of memory anti-tetanus and anti-HBV IgG secreting B cells >0.1% of total IgG secreting B cells. In conclusion, SSNS children at disease onset pre-immunosuppressive therapy showed a competent immune and vaccine response against tetanus and HBV, which can be correctly evaluated by quantification of antigen-specific memory B cells rather than by measuring serum IgG levels. This approach allows early identification of the impairment of immune and vaccine competence, which may derive from protracted use of different immunosuppressive drugs during disease course.
Keywords: ELISPOT; IgG; immune competence; pediatric nephrology; steroid-sensitive nephrotic syndrome; vaccine competence.
Copyright © 2021 Colucci, Piano Mortari, Zotta, Corrente, Concato, Carsetti, Emma and Vivarelli.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Heslan JM, Lautie JP, Intrator L, Blanc C, Lagrue G, Sobel AT. Impaired IgG synthesis in patients with the nephrotic syndrome. Clin Nephrol. (1982) 18:144–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources