

The Manipulation of the Lipid Mediator Metabolism as Adjunct Host-Directed Therapy in Tuberculosis
- PMID: 33777003
- PMCID: PMC7994275
- DOI: 10.3389/fimmu.2021.623941
The Manipulation of the Lipid Mediator Metabolism as Adjunct Host-Directed Therapy in Tuberculosis
Abstract
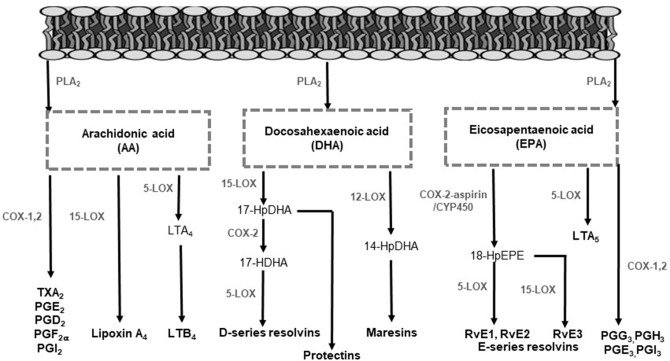
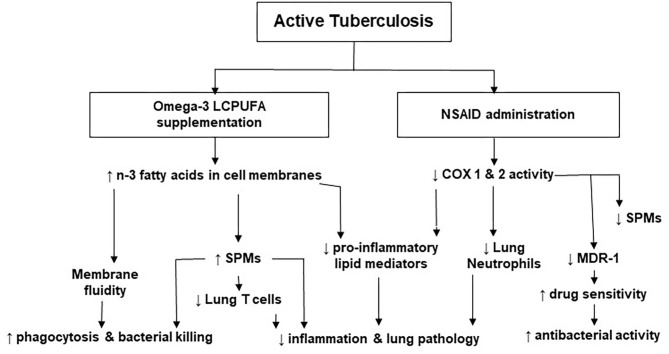
Host-directed therapies (HDTs) enhance the host response to tuberculosis (TB) infection to reduce disease severity. For instance, the manipulation of lipid mediator production diminishes the hyperactive immune response which is a known pathological feature of TB that generates lung tissue damage. Non-steroidal anti-inflammatory drugs (NSAIDs) and omega-3 long-chain polyunsaturated fatty acids (n-3 LCPUFA) are examples of such HDTs. In this mini-review, we recapitulate the literature available on the effects of NSAIDs and n-3 LCPUFA in TB as well as the immunological pathways underpinning these effects. Many NSAIDs have a great deal of data describing their effects and safety and in many jurisdictions are inexpensive, and sold over the counter in neighborhood convenience stores and supermarkets. The potential benefits of NSAIDs in TB are well-documented in pre-clinical studies. The reduction of pro-inflammatory lipid mediator production by inhibiting cyclooxygenase (COX) pathways with NSAIDs has been found to improve lung histopathology, bacterial control, and survival. Additionally, n-3 LCPUFA and its novel bioactive metabolites produced by COX and lipoxygenase (LOX) have been identified as safe and effective pro-resolving and antibacterial pharmaconutrients. Nevertheless, heterogeneous results have been reported in pre-clinical TB studies. Recently, the importance of the correct timing of NSAIDs and n-3 LCPUFA administration in TB has also been highlighted. This mini-review will provide a better understanding of the potential contribution of these therapies toward reducing inflammatory lung damage and improving bactericidal activity, especially during later stages of TB infection. It further highlights that clinical trials are required to confirm benefit and safety in TB patients.
Keywords: cyclooxygenase; lipid mediators; lipoxygenase; non-steroidal anti-inflammatory drugs; omega-3 polyunsaturated fatty acids; pharmaconutrition; tuberculosis.
Copyright © 2021 Nienaber, Hayford, Variava, Martinson and Malan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- WHO . Global Tuberculosis Report. Geneva: World Heatlh Organization; (2019).
-
- Dheda K, Gumbo T, Maartens G, Dooley KE, McNerney R, Murray M, et al. The epidemiology, pathogenesis, transmission, diagnosis, and management of multidrug-resistant, extensively drug-resistant, and incurable tuberculosis. Lancet Respir Med. (2017) 5:291–360. 10.1016/S2213-2600(17)30079-6 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources