

The translabyrinthine approach in residency training. "Step by step" surgical anatomy from the dissection laboratory to the operative room
- PMID: 33777123
- PMCID: PMC7985018
- DOI: 10.1016/j.joto.2020.09.002
The translabyrinthine approach in residency training. "Step by step" surgical anatomy from the dissection laboratory to the operative room
Abstract
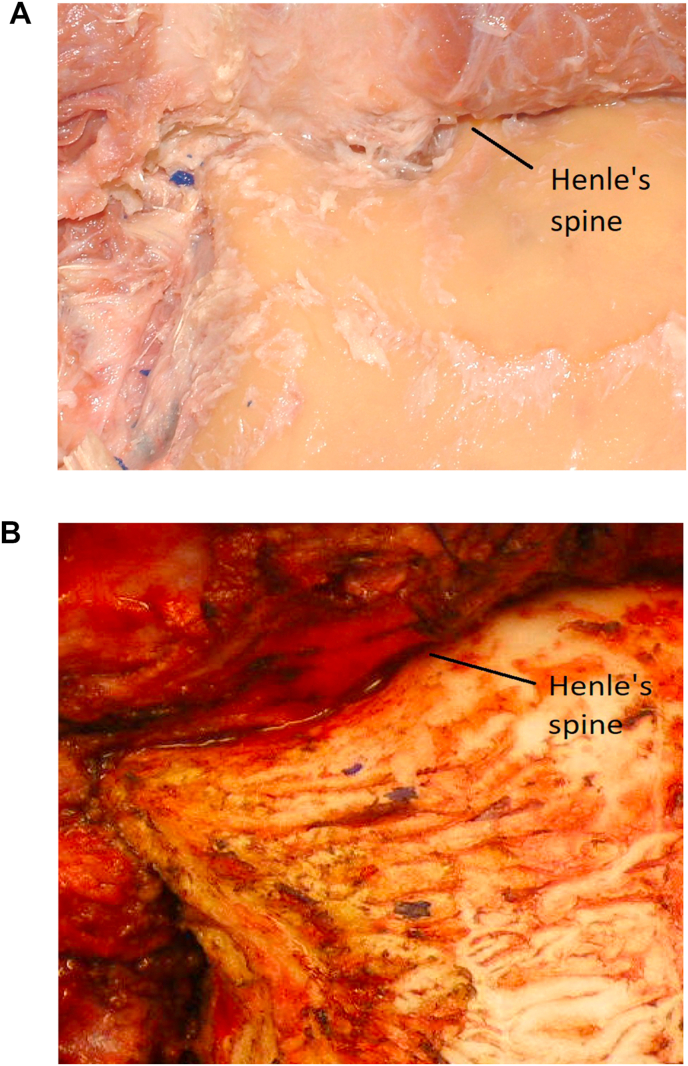
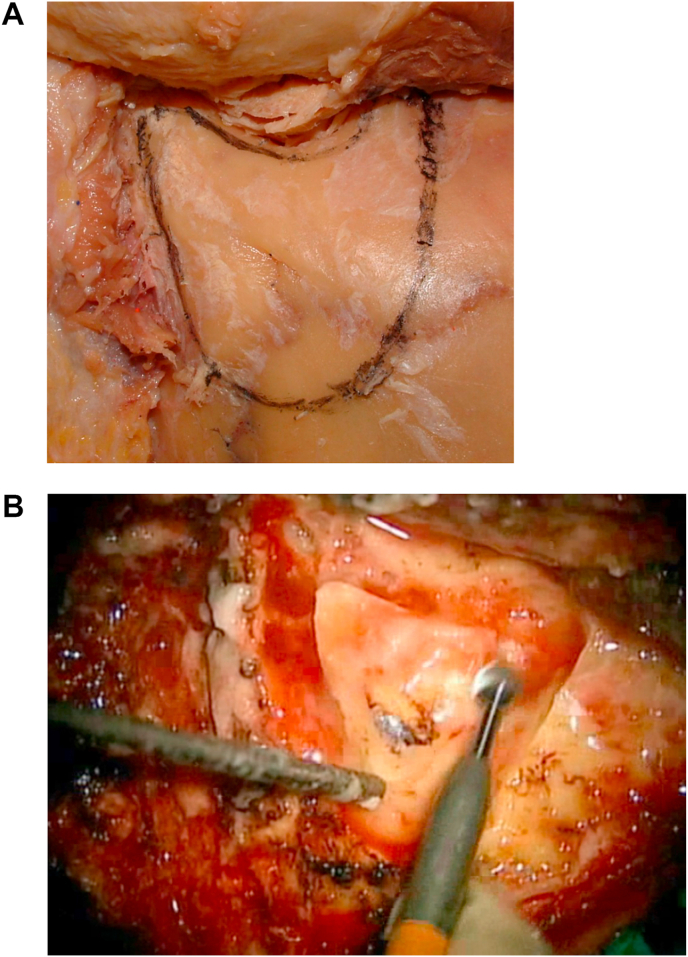
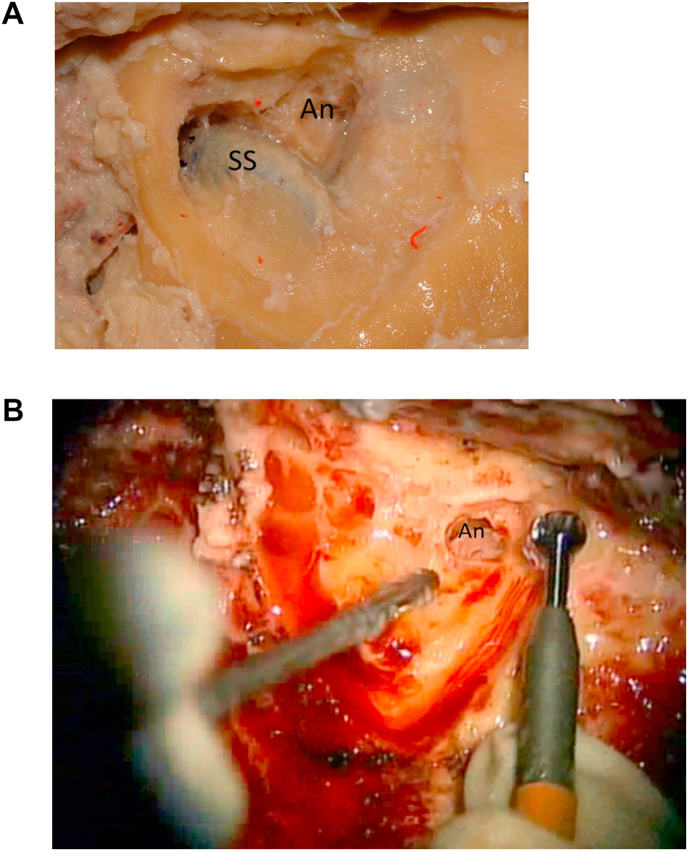
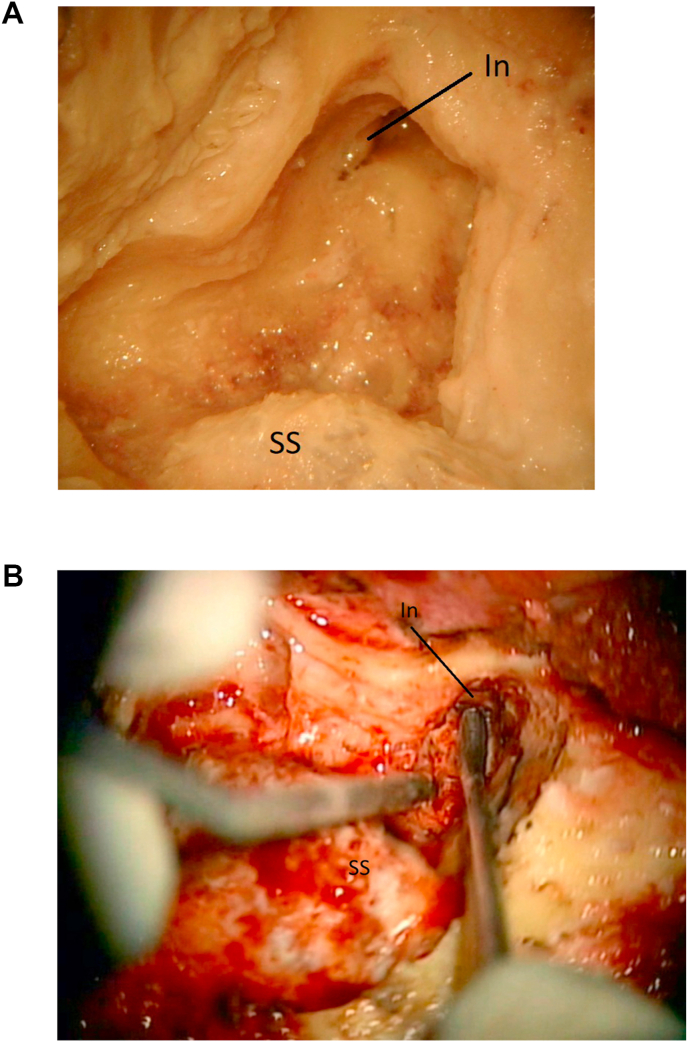
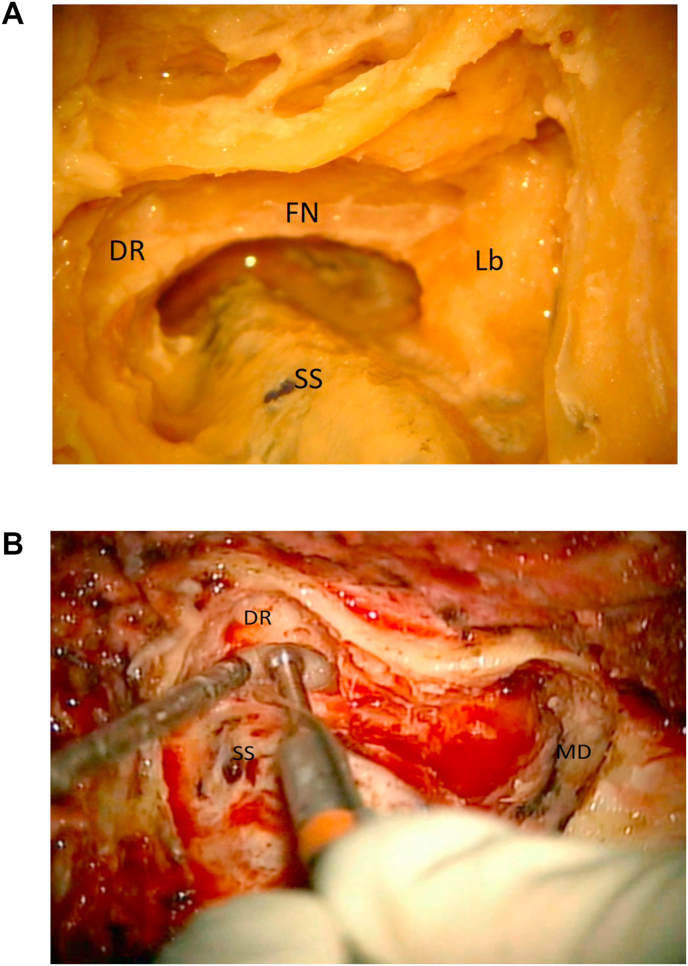
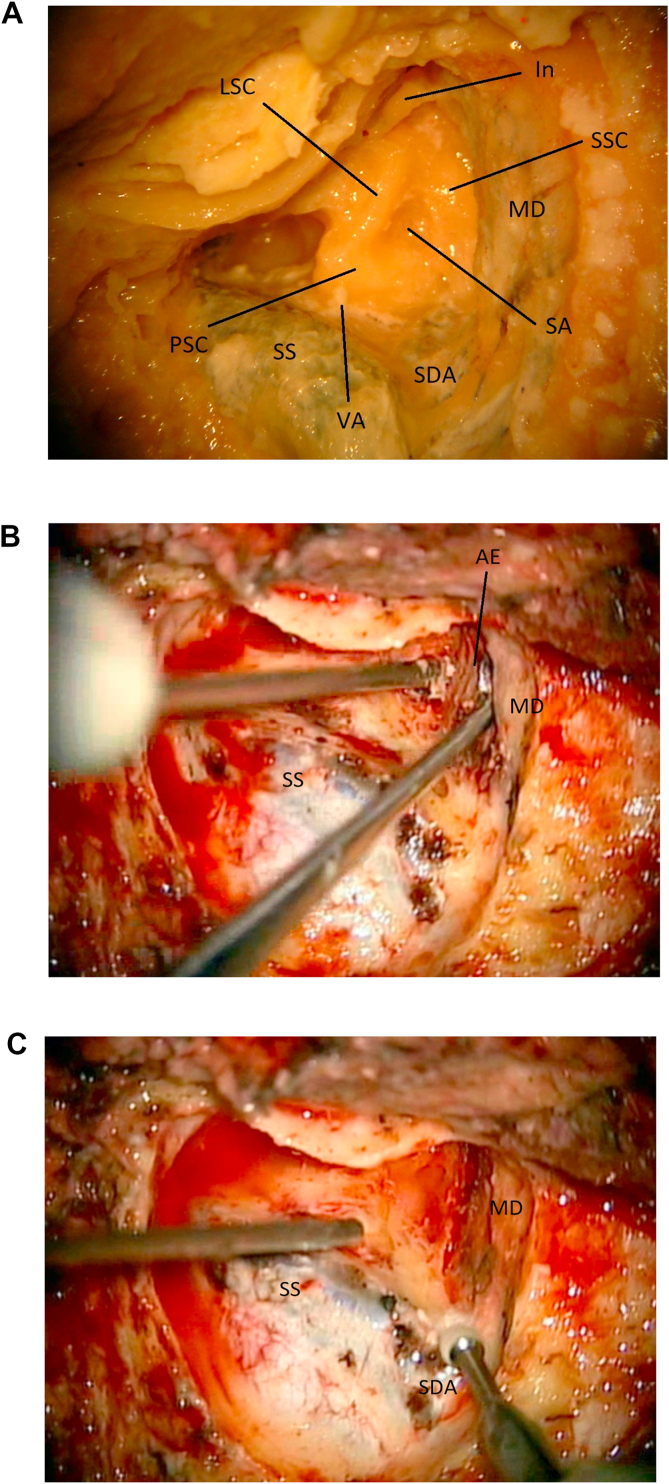
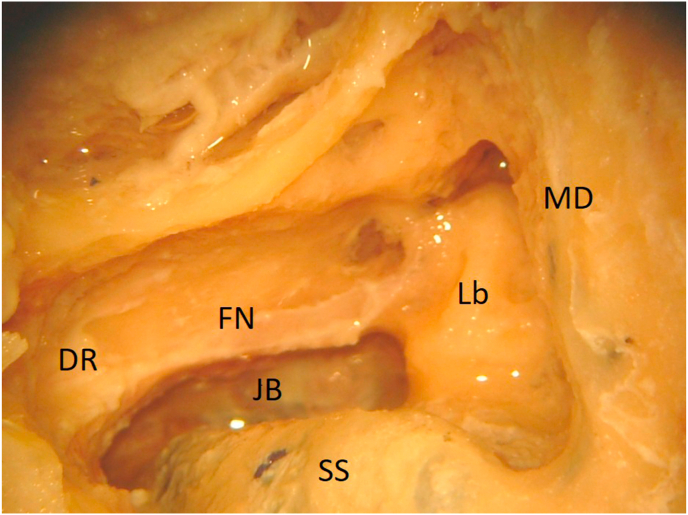
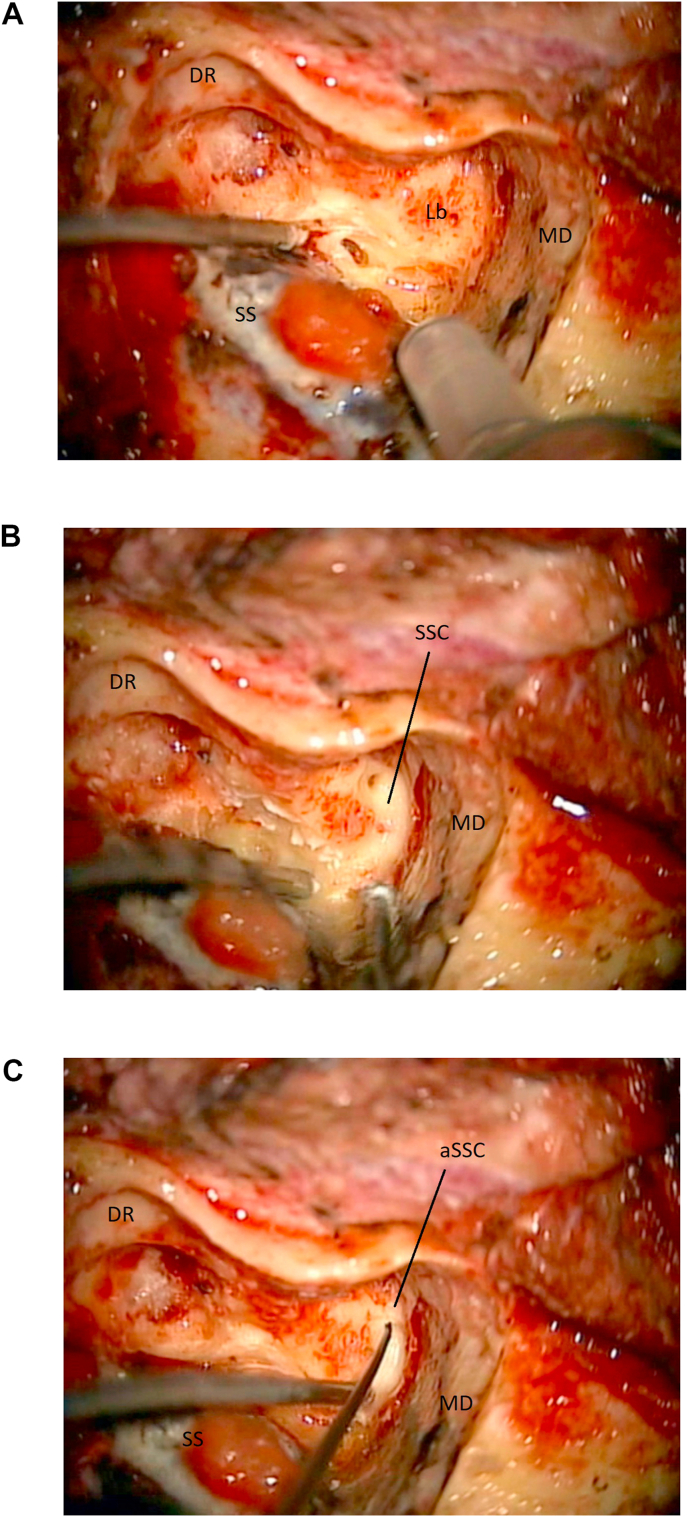
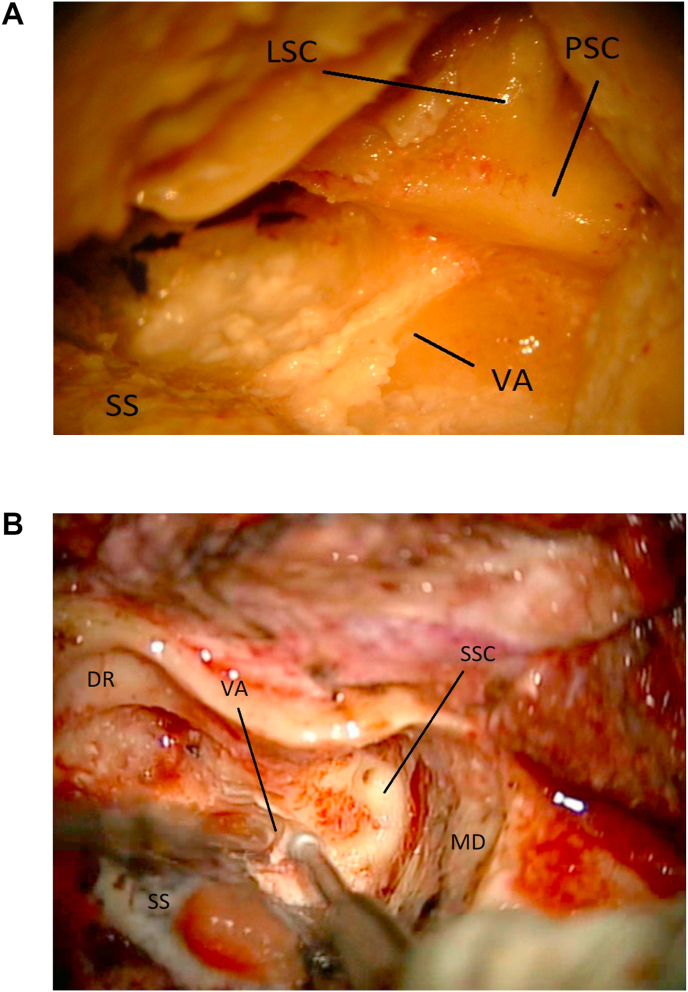
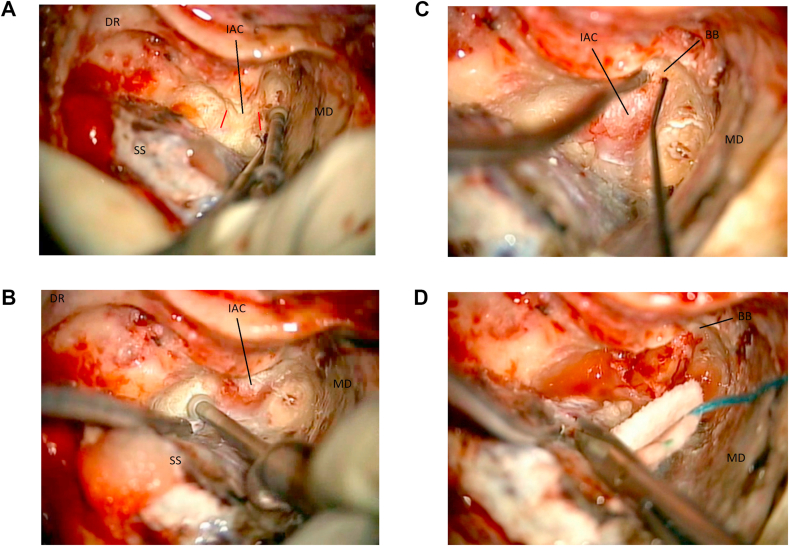
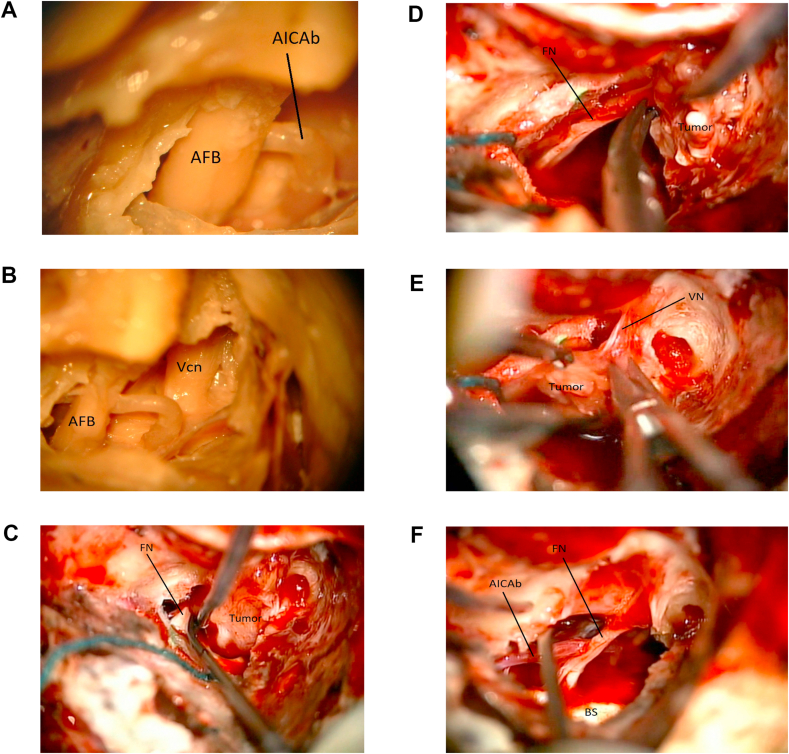
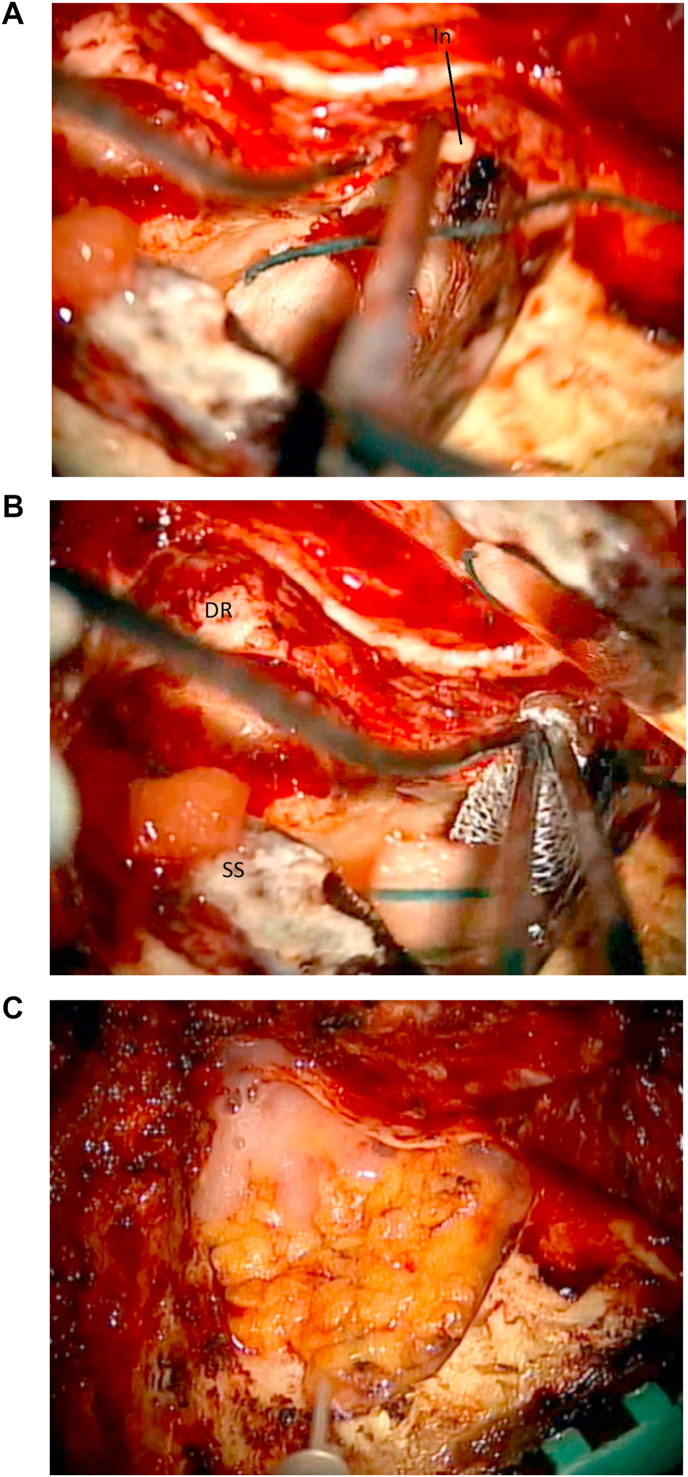
Surgical anatomy training in a dedicated research laboratory and attendance to focused "hands-on" dissection courses are of high educational importance in order to acquire and maintain surgical expertise in skull base surgery, both for young and more experienced surgeons. Nevertheless, transitioning surgical skills and anatomic knowledge from the laboratory to the operative room it is not free of challenges, especially during skull base approaches where the three-dimensional surgical orientation can be quite complex. We present a "step-by-step" and "side-by-side" surgical anatomy report on a translabyrinthine approach that was practiced in the laboratory then performed in the operative room by the surgical team, and we compare surgical anatomy exposures while discussing intraoperative techniques, nuances and challenges, both in the laboratory and the operative room.
Keywords: EMG, electromyogram; OR, operative room; Skull base surgery; TL, translabyrinthine; Translabyrinthine approach; Vestibular schwannomas.
© 2020 PLA General Hospital Department of Otolaryngology Head and Neck Surgery. Production and hosting by Elsevier (Singapore) Pte Ltd.
Figures

References
-
- Ammar M.B., Piccirillo E., Topsakal V., Taibah A., Sanna M. Surgical results and technical refinements in translabyrinthine excision of vestibular schwannomas: the gruppo otologico experience. Neurosurgery. Jun 2012;70(6):1481–1491. - PubMed
-
- Cushing H. WB Saunders Co; Philadelphia, PA: 1917. Tumors of the Nervus Acusticus and the Syndrome of the Cerebellopontine Angle.
-
- Cushing H. Further concerning the acoustic neuromas. Laryngoscope. 1921;31:209–228.
-
- Hirsch B.E., Cass S.P., Sekhar L.N., Wright D.C. Translabyrinthine approach to skull base tumors with hearing preservation. Am. J. Otol. 1993;14:533–543. - PubMed
-
- House W.F. Transtemporal bone microsurgical removal of acoustic neuromas. Report of cases. Arch. Otolaryngol. 1964;80:617–667. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
