

Anemia of cardiorenal syndrome
- PMID: 33777494
- PMCID: PMC7983020
- DOI: 10.1016/j.kisu.2020.12.001
Anemia of cardiorenal syndrome
Abstract
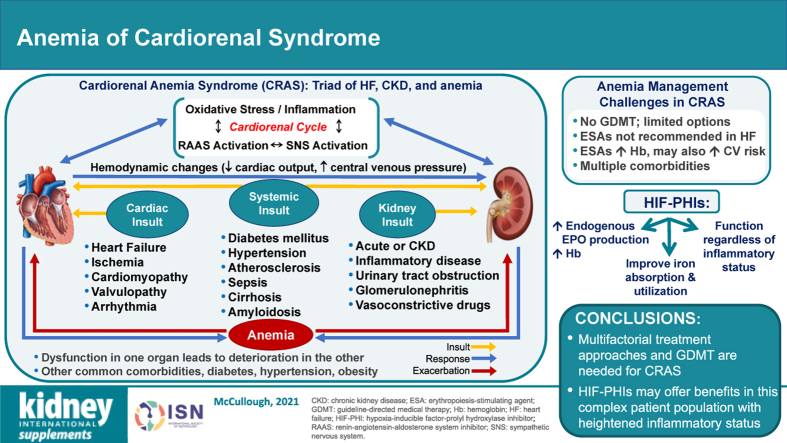
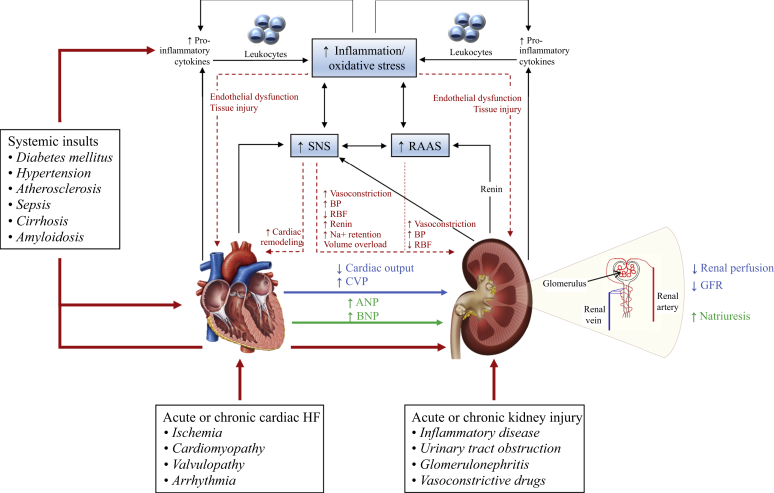
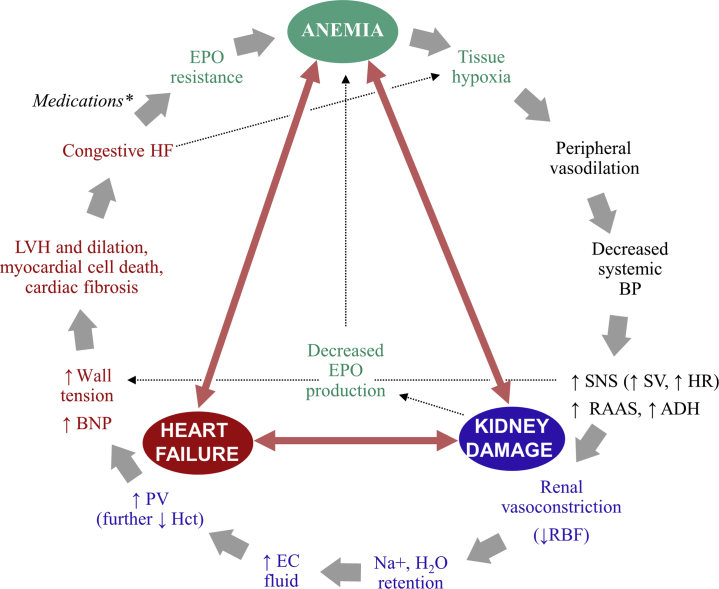
Cardiorenal syndrome includes a spectrum of disorders of the kidneys and heart in which loss of function in one organ contributes to reduced function in the other organ. Cardiorenal syndrome is frequently complicated by comorbid anemia, which leads to reciprocal and progressive cardiac and renal deterioration. The triad of heart failure, chronic kidney disease (CKD), and anemia is termed cardiorenal anemia syndrome (CRAS). There are currently no evidence-based recommendations for managing patients with CRAS; however, the treatment of these patients is multifactorial. Not only must the anemia be controlled, but heart failure and kidney injury must be addressed, in addition to other comorbidities. Intravenous iron and erythropoiesis-stimulating agents are the mainstays of treatment for anemia of CKD, addressing both iron and erythropoiesis deficiencies. Since erythropoiesis-stimulating agent therapy can be associated with adverse outcomes at higher doses in patients with CKD and is not used in routine practice in patients with heart failure, treatment options for managing anemia in patients with CRAS are limited. Several new therapies, particularly the hypoxia-inducible factor-prolyl hydroxylase inhibitors, are currently under clinical development. The hypoxia-inducible factor-prolyl hydroxylase inhibitors have shown promising results for treating anemia of CKD in clinical trials and may confer benefits in patients with CRAS, potentially addressing some of the limitations of erythropoiesis-stimulating agents. Updated clinical practice guidelines for the screening and management of anemia in cardiorenal syndrome, in light of potential new therapies and clinical evidence, would improve the clinical outcomes of patients with this complex syndrome.
Keywords: cardiovascular disease; chronic kidney disease; erythropoiesis-stimulating agents; heart failure; hypoxia-inducible factor–prolyl hydroxylase inhibitor; iron deficiency.
© 2021 International Society of Nephrology. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Rangaswami J., Bhalla V., Blair J.E.A. Cardiorenal syndrome: classification, pathophysiology, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation. 2019;139:e840–e878. - PubMed
-
- 2018 USRDS Annual Data Report: Executive Summary. Am J Kidney Dis. 2019;73:A9–A22.
-
- Go A.S., Chertow G.M., Fan D. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
