

High sensitivity of PD-L1 analysis from pleural effusion in nonsmall cell lung cancer
- PMID: 33778051
- PMCID: PMC7983225
- DOI: 10.1183/23120541.00787-2020
High sensitivity of PD-L1 analysis from pleural effusion in nonsmall cell lung cancer
Abstract
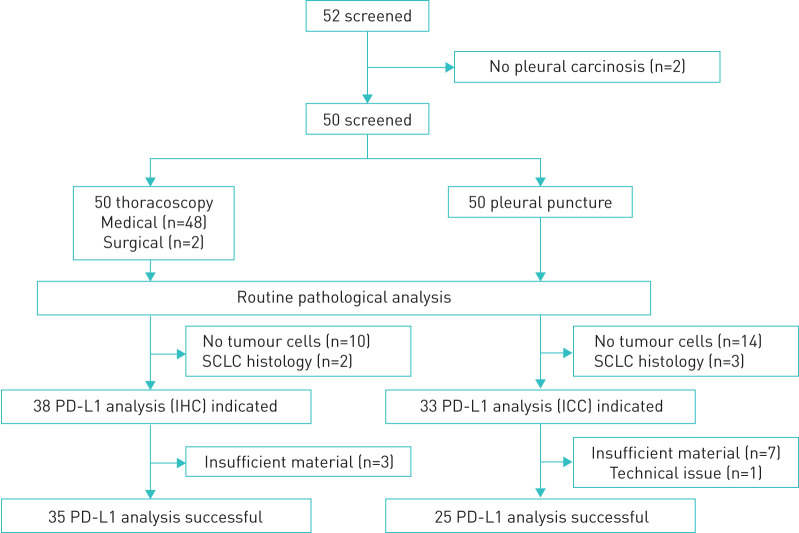
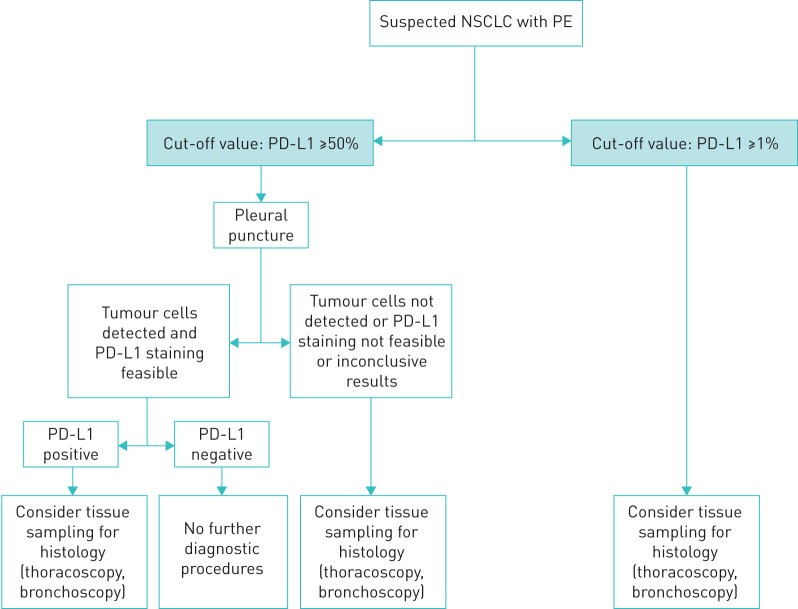
Background: Programmed cell death protein 1 (PD-1)/programmed cell death protein ligand 1 (PD-L1) immune checkpoint inhibitors have been approved for monotherapy of metastatic nonsmall cell lung cancer (mNSCLC) depending on tumour cells' PD-L1 expression. Pleural effusion is common in mNSCLC. The significance of immunocytochemistry PD-L1 analysis from pleural effusion samples is unclear. Aim: The aim of the study was to analyse the sensitivity regarding immunocytochemistry PD-L1 analysis of pleural effusion in NSCLC as compared to immunohistochemistry of pleural biopsies. Patients and Methods: Fifty consecutive subjects (17 female, median age 72.5 years, seven never-smokers) were enrolled in this prospective controlled two-centre study. Inclusion criteria were pleural effusion, suspected or known lung cancer, indication for pleural puncture and thoracoscopy, and written informed consent. Immunocytochemistry and immunohistochemistry PD-L1 analyses were performed with the Dako-PDL1-IHC-22C3pharmDx assay. Analysis for sensitivity, specificity, and positive and negative predictive value was performed for PD-L1 detection from pleural effusion. Results: 50 subjects underwent pleural puncture and thoracoscopy. Pathological diagnoses were lung cancer (48), lymphoma (1) and mesothelioma (1). Sensitivity, specificity, positive predictive value and negative predictive value of PD-L1-testing with expression ≥50% defined as positive were 100% (95% CI 46-100%), 63% (36-84%), 45% (18-75%) and 100% (66-100%), and with expression ≥1% defined as positive 86% (56-97%), 43% (12-80%), 75% (47-92%) and 60% (17-93%). Conclusion: PD-L1 analysis in tumour-positive pleural effusion samples shows a very high sensitivity and negative predictive value, especially regarding PD-L1 expression levels ≥50% (European Medicines Agency approval). Negative results are reliable and help in the decision against a first-line checkpoint inhibitor monotherapy. However, a 1% cut-off level (United States Food and Drug Administration approval) leads to a markedly lower negative predictive value, making other invasive procedures necessary (NCT02855281).
Copyright ©ERS 2021.
Conflict of interest statement
Conflict of interest: L. Hagmeyer reports grants from MSD Sharp & Dohme GmbH, Haar, Germany, during the conduct of the study; and grants from AstraZeneca, from Roche, from Boehringer Ingelheim and from Pfizer, outside the submitted work. Conflict of interest: S. Schäfer reports personal fees from Boehringer Ingelheim and BMS outside the submitted work. Conflict of interest: M. Engels has nothing to disclose. Conflict of interest: A. Pietzke-Calcagnile has nothing to disclose. Conflict of interest: M. Treml has nothing to disclose. Conflict of interest: S-D. Herkenrath has nothing to disclose. Conflict of interest: M. Heldwein has nothing to disclose. Conflict of interest: K. Hekmat has nothing to disclose. Conflict of interest: S. Matthes has nothing to disclose. Conflict of interest: A. Scheel has nothing to disclose. Conflict of interest: J. Wolf reports personal fees from Abbvie, AstraZeneca and Blueprint, grants and personal fees from BMS, personal fees from Böhringer, Chugai and Ignyta, grants and personal fees from Jannsen, personal fees from Lilly and Loxo, grants and personal fees from MSD, Novartis and Pfizer, and personal fees from Roche and Takeda, outside the submitted work. Conflict of interest: R. Buettner has nothing to disclose. Conflict of interest: W. Randerath reports speaking fees and travel grants from Philips Respironics, Heinen and Löwenstein, Resmed, Bayer Vital, Bioprojet, and Vanda Pharma, outside the submitted work.
Figures
Similar articles
-
Expression and clinical significance of programmed death ligand-1 evaluated by 22C3 antibody in pleural effusion metastatic non-small-cell lung cancer.Cytojournal. 2024 Dec 20;21:70. doi: 10.25259/Cytojournal_59_2024. eCollection 2024. Cytojournal. 2024. PMID: 39917015 Free PMC article.
-
PD-L1 detection in histology specimens and matched pleural fluid cell blocks of patients with NSCLC.Respirology. 2019 Dec;24(12):1198-1203. doi: 10.1111/resp.13614. Epub 2019 Jun 17. Respirology. 2019. PMID: 31209954
-
[Correlation between the Expression of PD-L1 in Pleural Effusion of Lung Adenocarcinoma and the Clinicopathological Features and Molecular Changes].Zhongguo Fei Ai Za Zhi. 2020 Mar 20;23(3):150-155. doi: 10.3779/j.issn.1009-3419.2020.03.03. Zhongguo Fei Ai Za Zhi. 2020. PMID: 32209183 Free PMC article. Chinese.
-
Predictive biomarkers for programmed death-1/programmed death ligand immune checkpoint inhibitors in nonsmall cell lung cancer.Curr Opin Oncol. 2016 Mar;28(2):122-9. doi: 10.1097/CCO.0000000000000263. Curr Opin Oncol. 2016. PMID: 26756384 Review.
-
[Efficacy of PD-1/PD-L1 immune checkpoint inhibitors and PD-L1 testing in thoracic cancers].Ann Pathol. 2017 Feb;37(1):61-78. doi: 10.1016/j.annpat.2016.12.009. Epub 2017 Feb 3. Ann Pathol. 2017. PMID: 28162296 Review. French.
Cited by
-
Evaluation of PD-1 and interleukin-10-receptor expression by T lymphocytes in malignant and benign pleural effusions.Clin Exp Med. 2024 Sep 26;24(1):228. doi: 10.1007/s10238-024-01485-y. Clin Exp Med. 2024. PMID: 39325190 Free PMC article.
References
-
- Rizvi N, Mazières J, Planchard D. Safety and clinical activity of MK-2475 as initial therapy in patients with advanced nonsmall cell lung cancer (NSCLC). J Clin Oncol 2014; 32: Suppl. 15, 8007.
-
- Garon E, Gandhi L, Rizvi N. LBA43 - Antitumor Activity of Pembrolizumab (Pembro; Mk-3475) and Correlation with Programmed Death Ligand 1 (Pd-L1) Expression in a Pooled Analysis of Patients (Pts) with Advanced Non–Small Cell Lung Carcinoma (Nsclc). Ann Oncol 2014; 25, Suppl. 5: v1–v41. doi:10.1093/annonc/mdu438.51. - DOI
-
- Rahman NM, Ali NJ, Brown G, et al. . Local anaesthetic thoracoscopy: British Thoracic Society Pleural Disease Guideline 2010. Thorax 2010; 65: Suppl. 2, ii54–ii60. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials