

Factors for Increased Hospital Stay and Utilization of Post -Acute Care Facilities in Geriatric Orthopaedic Fracture Patients
- PMID: 33778118
- PMCID: PMC7957104
- DOI: 10.22038/abjs.2020.46476.2276
Factors for Increased Hospital Stay and Utilization of Post -Acute Care Facilities in Geriatric Orthopaedic Fracture Patients
Abstract
Background: This study aims to determine the extent of utilization of health care resources in the geriatric fracture population and to identify factors associated with burden on resources.
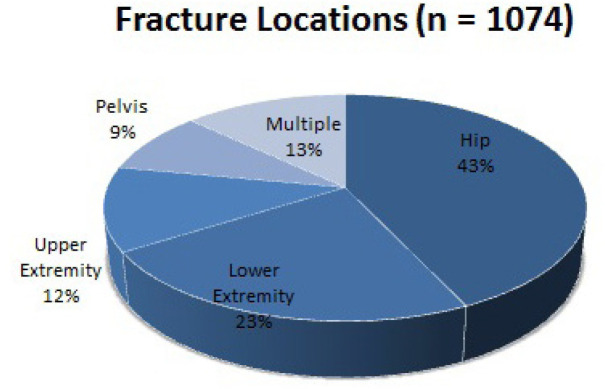
Methods: This is a retrospective study of 1074 patients ≥65 years admitted to an orthopaedic service for a long bone fracture between July 2014 - June 2015. Outcomes were hospital length of stay (LOS), discharge disposition, and post-acute care facility LOS. Secondarily, readmission rates and mortality were assessed. Multivariable regression was performed to identify factors associated with utilization.
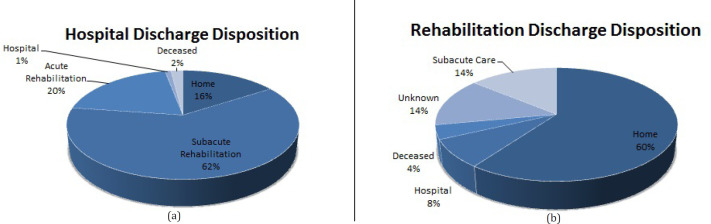
Results: Prior to injury, 96% of patients lived at home and 50% ambulated independently. Median hospital LOS was 5 days (IQR 3 - 7). 878 patients were discharged to a rehabilitation facility, with 45% being discharged <20 days. Ten percent of patients (n = 108) were re-admitted <90 days of their discharge. 924 patients were still alive one year after the injury. Higher Charlson Comorbidity Index (CCI) (P=0.048), male sex (P<0.001), pre-injury use of an ambulatory device (P = 0.006), and undergoing surgical treatment (P<0.001) were associated with longer hospital LOS. Older age (P<0.001), pre-injury ambulatory device (P=0.001), and surgery (P=0.012) were risk factors for requiring discharge to another inpatient facility. Older age (P<0.001), pre-injury ambulatory aid (P<0.001), and pre-existing immobility (P<0.001) were independent risk factors for LOS >20 days in a rehabilitation facility. Discharge home was not found to be associated with an increase in 1-year mortality after adjusting for age, CCI, sex, fracture location, and surgery (P=0.727). Shorter LOS in rehabilitation facilities (<20 days) was also not associated with an increase in 1-year mortality (P=0.520).
Conclusion: Elderly fracture patients utilize a significant amount of post-acute care resources and age, CCI, surgery, fracture location, pre-injury ambulatory status, and pre-injury living status were found to be associated with the use of these resources.
Keywords: Bundled payments; Fracture; Geriatric; Healthcare utilization; Length of stay; Post-acute care; Rehabilitation.
Figures
References
-
- U.S. Census Bureau. The Older Population: 2010. [Internet]. [Place unknown]: 2010 Census Briefs; Nov 2011. [[cited 2017 Jul 5]]. Available from: https://www.census.gov/newsroom/releases/archives/2010_census/cb11-cn192....
-
- Centers for Disease Control and Prevention. Incidence and costs to Medicare of fractures among Medicare beneficiaries aged> or= 65 years--United States, July 1991-June 1992. MMWR: Morbidity and mortality weekly report. 1996;45(41):877–83. - PubMed
-
- Porter ME. A strategy for health care reform—toward a value-based system. N Engl J Med. 2009;361(2):109–12. - PubMed
-
- Porter ME, Lee TH. The Strategy That Will Fix Health Care. Harv Bus Rev . 2013;91(10):50–70. - PubMed
-
- Lee VS, Kawamoto K, Hess R, Park C, Young J, Hunter C, et al. Implementation of a Value-Driven Outcomes Program to Identify High Variability in Clinical Costs and Outcomes and Association With Reduced Cost and Improved Quality. JAMA. 2016;316(10):1061–72. - PubMed
LinkOut - more resources
Full Text Sources