

Plan switching among Medicare Advantage beneficiaries with Alzheimer's disease and other dementias
- PMID: 33778149
- PMCID: PMC7987817
- DOI: 10.1002/trc2.12150
Plan switching among Medicare Advantage beneficiaries with Alzheimer's disease and other dementias
Abstract
Introduction: Patients with Alzheimer's disease and related dementias (ADRD) face substantial challenges in selecting, and remaining enrolled in, health insurance. Little is known about how patients with ADRD experience the Medicare Advantage (MA) program.
Methods: We used, hospital, outpatient, and post-acute care data to identify MA beneficiaries with and without ADRD in 2014. Multinomial logit models estimated the percentage of people who disenrolled to traditional Medicare (TM) or switched to a different MA plan in 2015.
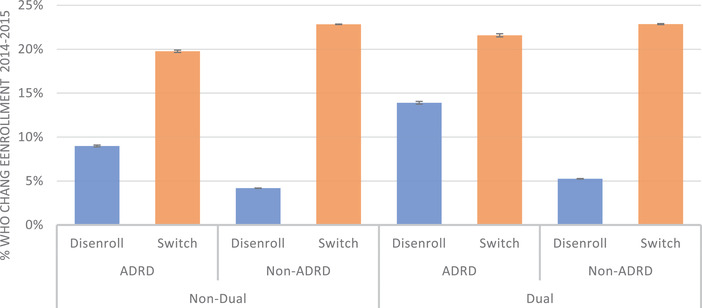
Results: Among non-dually eligible beneficiaries, 9.0% (95% confidence interval [CI]: 8.0, 9.1) with ADRD disenrolled while 19.7% (95% CI: 19.6, 19.9) switched plans within MA compared to a disenrollment rate of 4.2% (95% CI: 4.2, 4.2) and switching rate of 22.8% (95% CI: 22.9, 22.8) for persons without ADRD.
Discussion: MA enrollees with ADRD tend to disenroll at substantially higher rates than those without ADRD. This may be indicative of their care needs not being met in the program.
Keywords: Medicare; Medicare Advantage; health insurance.
© 2021 The Authors. Alzheimer's & Dementia: Translational Research & Clinical Interventions published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
Vincent Mor is chair of the scientific advisory board and a consultant at NaviHealth, Inc., as well as former director of PointRight, Inc., where he holds < 1% equity. All other authors have no interests to declare.
Figures
References
-
- Neuman P, Jacobson GA. Medicare advantage checkup. N Engl J Med. 2018;379:2163‐2172. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous