

COVID-19: A Multimodality Review of Radiologic Techniques, Clinical Utility, and Imaging Features
- PMID: 33778588
- PMCID: PMC7325394
- DOI: 10.1148/ryct.2020200210
COVID-19: A Multimodality Review of Radiologic Techniques, Clinical Utility, and Imaging Features
Abstract
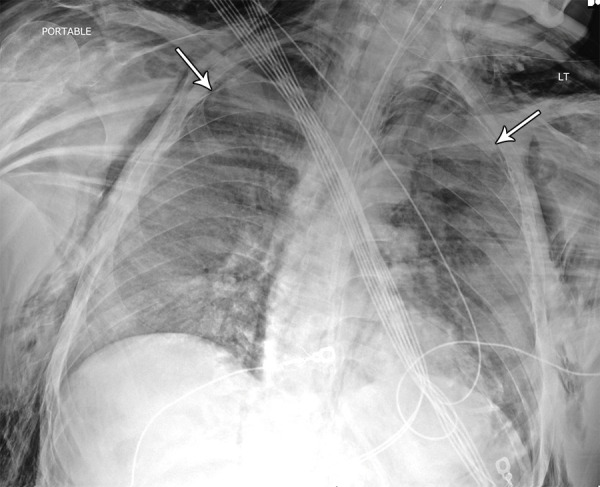
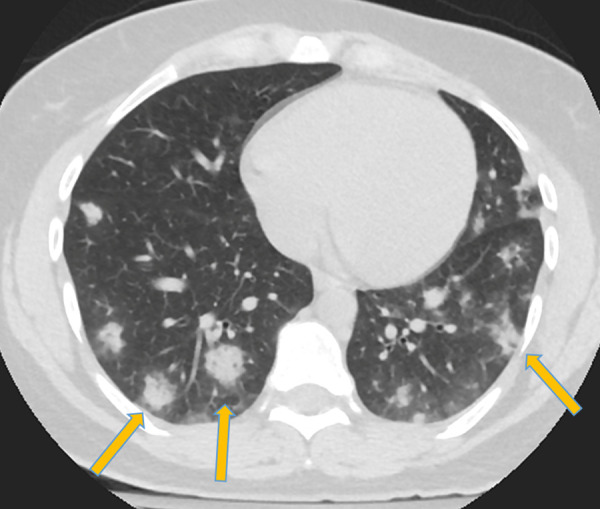
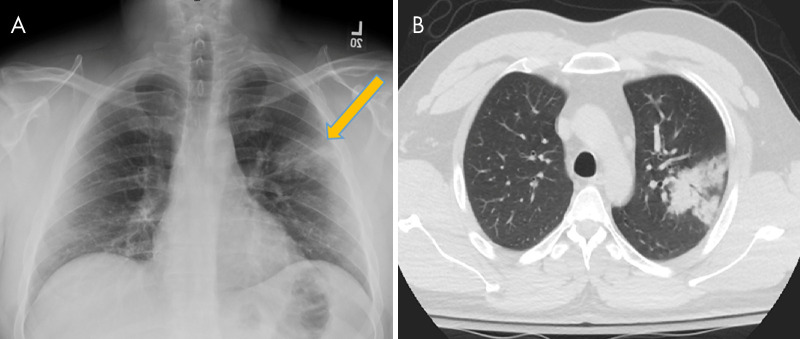
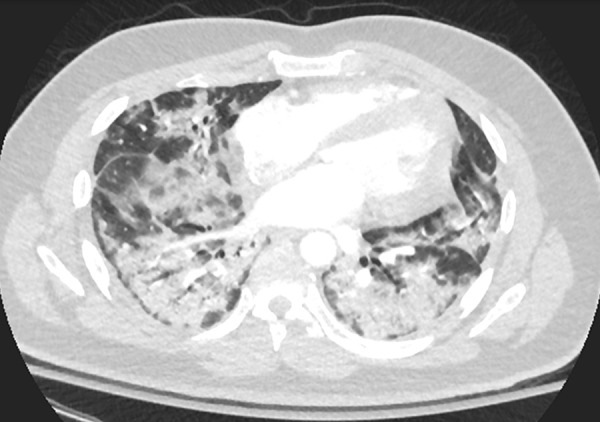
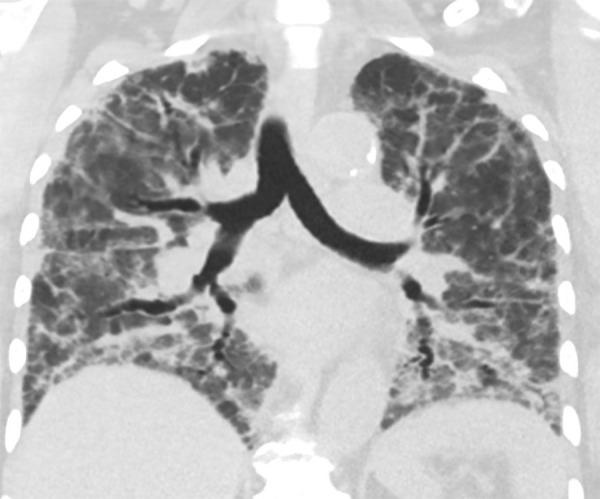
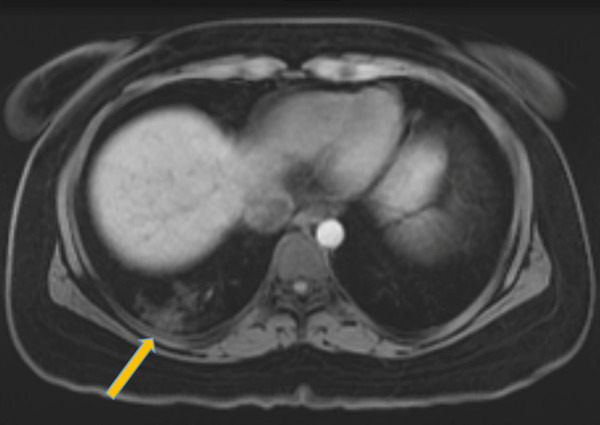
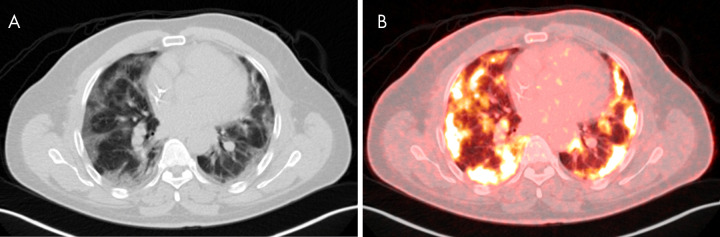
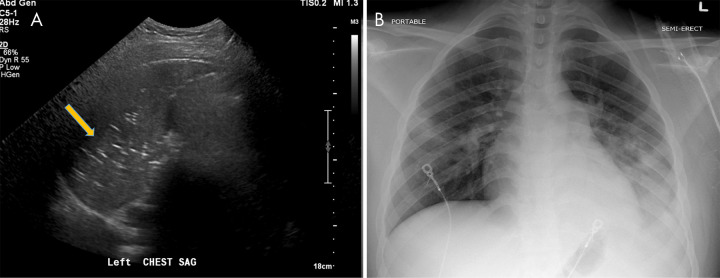
In this article we will review the imaging features of coronavirus disease 2019 (COVID-19) across multiple modalities, including radiography, CT, MRI, PET/CT, and US. Given that COVID-19 primarily affects the lung parenchyma by causing pneumonia, our directive is to focus on thoracic findings associated with COVID-19. We aim to enhance radiologists' understanding of this disease to help guide diagnosis and management. Supplemental material is available for this article. © RSNA, 2020.
2020 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: S.M. disclosed no relevant relationships. J.W. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author is member of National Cancer Institute’s Physician Data Query board for cancer screening and prevention, unrelated to the topic of this article; participation is not reimbursed but travel to meetings is reimbursed. Other relationships: disclosed no relevant relationships. S.Z.M. disclosed no relevant relationships. D.T. disclosed no relevant relationships. N.V. disclosed no relevant relationships. M.F. disclosed no relevant relationships. M.A.C. disclosed no relevant relationships. J.D. disclosed no relevant relationships. C.E. disclosed no relevant relationships. A.J. disclosed no relevant relationships. M.C. disclosed no relevant relationships. A.B. disclosed no relevant relationships.
Figures

References
-
- Coronavirus COVID-19 Global Cases by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. (JHU). The Johns Hopkins University School of Medicine. https://coronavirus.jhu.edu/map.html. Published 2020. Accessed March 2020.
-
- Buonsenso D, Piano A, Raffaelli F, Bonadia N, de Gaetano Donati K, Franceschi F. Point-of-Care Lung Ultrasound findings in novel coronavirus disease-19 pnemoniae: a case report and potential applications during COVID-19 outbreak. Eur Rev Med Pharmacol Sci 2020;24(5):2776–2780. - PubMed
LinkOut - more resources
Full Text Sources
