

Diagnostic Accuracy of North America Expert Consensus Statement on Reporting CT Findings in Patients Suspected of Having COVID-19 Infection: An Italian Single-Center Experience
- PMID: 33778611
- PMCID: PMC7380122
- DOI: 10.1148/ryct.2020200312
Diagnostic Accuracy of North America Expert Consensus Statement on Reporting CT Findings in Patients Suspected of Having COVID-19 Infection: An Italian Single-Center Experience
Abstract
Purpose: To evaluate the diagnostic accuracy of the four standardized categories for CT reporting proposed by the Radiological Society of North America (RSNA) to support a faster triage compared with real-time reverse-transcription polymerase chain reaction (RT-PCR), which is the reference standard for suspected coronavirus disease 2019 (COVID-19), but has long reporting time (6-48 hours).
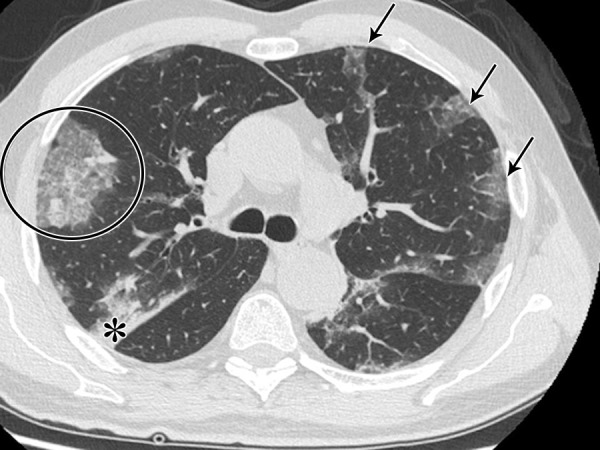
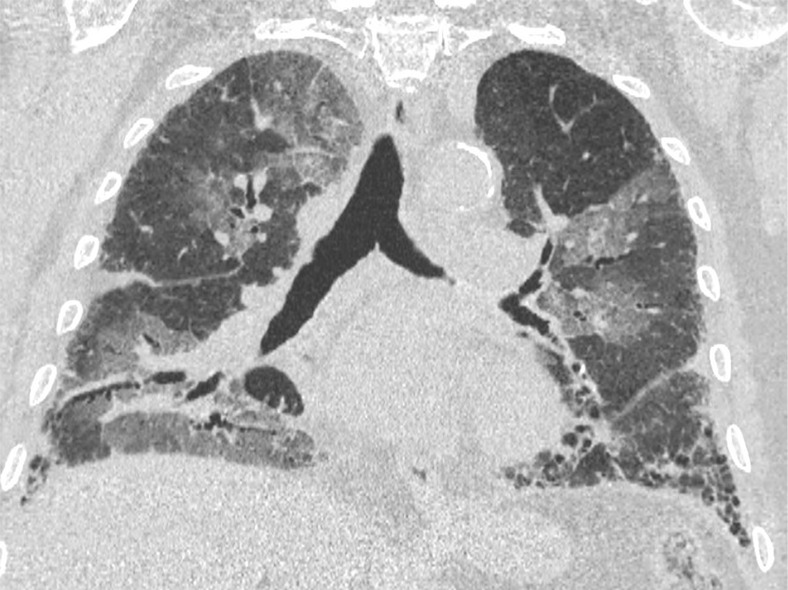
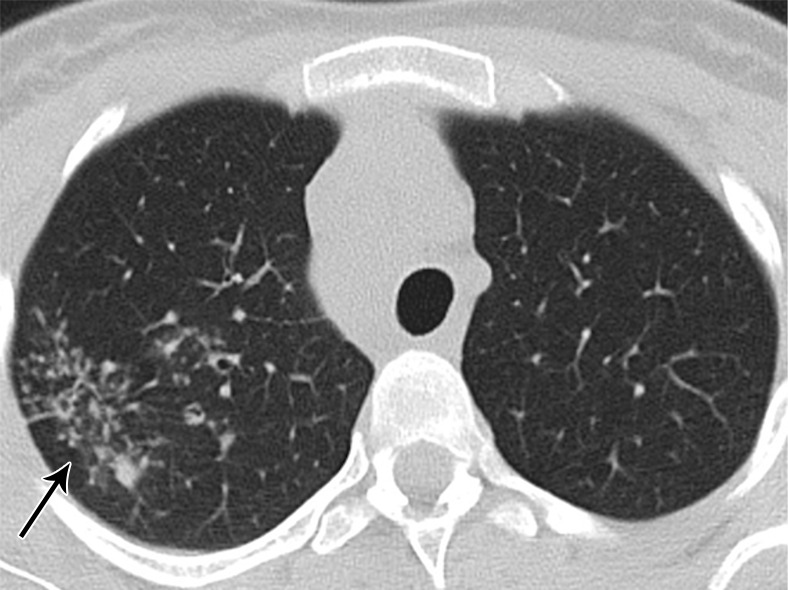
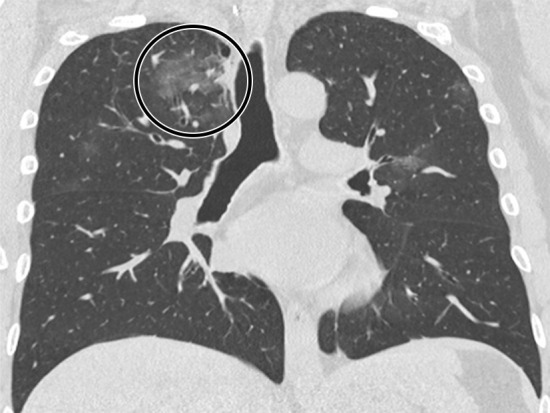
Materials and methods: A retrospective analysis of 569 thin-section CT examinations performed for patients suspected of having COVID-19 from February 27 to March 27, 2020 (peak of infection in Italy) was conducted. The imaging pattern was classified according to the statement by the RSNA as "typical," "indeterminate," "atypical," and "negative" and compared with RT-PCR for 460 patients. Interobserver variability in reporting between a senior and a junior radiologist was evaluated. Use of the vascular enlargement sign in indeterminate cases was also assessed.
Results: The diagnosis of COVID-19 was made in 45.9% (211/460) of patients. The "typical" pattern (n = 172) showed a sensitivity of 71.6%, a specificity of 91.6%, and a positive predictive value of 87.8% for COVID-19. The "atypical" (n = 67) and "negative" (n = 123) pattern demonstrated a positive predictive value of 89.6% and 86.2% for non-COVID-19, respectively. The "indeterminate" (n = 98) pattern was nonspecific, but vascular enlargement was most frequently found in patients with COVID-19 (86.1%; P < .001). Interobserver agreement was good for the "typical" and "negative" pattern and fair for "indeterminate" and "atypical" (κ = 0.5; P = .002).
Conclusion: In an epidemic setting, the application of the four categories proposed by the RSNA provides a standardized diagnostic hypothesis, strongly linked to the RT-PCR results for the "typical," "atypical," and "negative" pattern. In the "indeterminate" pattern, the analysis of the vascular enlargement sign could facilitate the interpretation of imaging features.© RSNA, 2020.
2021 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: F. Ciccarese disclosed no relevant relationships. F. Coppola disclosed no relevant relationships. D.S. disclosed no relevant relationships. G.L.G. disclosed no relevant relationships. V.L. disclosed no relevant relationships. A.P. disclosed no relevant relationships. C.D.B. disclosed no relevant relationships. C.B. disclosed no relevant relationships. R.G. disclosed no relevant relationships.
Figures







References
-
- WHO Coronavirus disease (COVID-2019) situation reports-147 . World Health Organization website. https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situatio.... Published June 15, 2020.
LinkOut - more resources
Full Text Sources
