

Implementation of the Radiological Society of North America Expert Consensus Guidelines on Reporting Chest CT Findings Related to COVID-19: A Multireader Performance Study
- PMID: 33778625
- PMCID: PMC7484923
- DOI: 10.1148/ryct.2020200276
Implementation of the Radiological Society of North America Expert Consensus Guidelines on Reporting Chest CT Findings Related to COVID-19: A Multireader Performance Study
Abstract
Background: RSNA expert consensus guidelines provide a framework for reporting CT findings related to COVID-19, but have had limited multireader validation.
Purpose: To assess the performance of the RSNA guidelines and quantify interobserver variability in application of the guidelines in patients undergoing chest CT for suspected COVID-19 pneumonia.
Materials and methods: A retrospective search from 1/15/20 to 3/30/20 identified 89 consecutive CT scans whose radiological report mentioned COVID-19. One positive or two negative RT-PCR tests for COVID-19 were considered the gold standard for diagnosis. Each chest CT scan was evaluated using RSNA guidelines by 9 readers (6 fellowship trained thoracic radiologists and 3 radiology resident trainees). Clinical information was obtained from the electronic medical record.
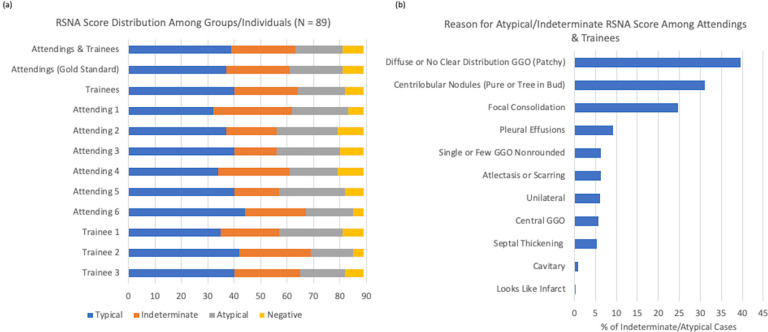
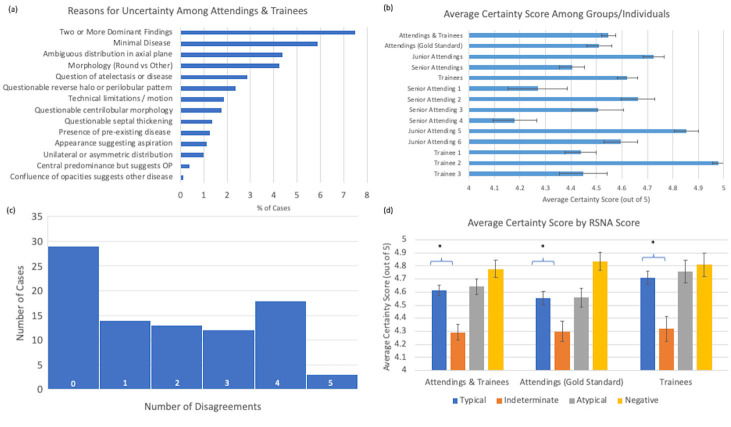
Results: There was strong concordance of findings between radiology training levels with agreement ranging from 60 to 86% among attendings and trainees (kappa 0.43 to 0.86). Sensitivity and specificity of "typical" CT findings for COVID-19 per the RSNA guidelines were on average 86% (range 72%-94%) and 80.2% (range 75-93%), respectively. Combined "typical" and "indeterminate" findings had a sensitivity of 97.5% (range 94-100%) and specificity of 54.7% (range 37-62%). A total of 163 disagreements were seen out of 801 observations (79.6% total agreement). Uncertainty in classification primarily derived from difficulty in ascertaining peripheral distribution, multiple dominant disease processes, or minimal disease.
Conclusion: The "typical appearance" category for COVID-19 CT reporting has an average sensitivity of 86% and specificity rate of 80%. There is reasonable interreader agreement and good reproducibility across various levels of experience.
2020 by the Radiological Society of North America, Inc.
Conflict of interest statement
Conflict of Interests and Disclosures: Dr. Little is a textbook author and editor for Elsevier and receives royalties for his prior work. Dr. Flores reports grant funding from the American College of Radiology Innovation Fund and the National Cancer Institute Research Diversity Supplement for work not related to this manuscript.
Figures
Similar articles
-
RSNA Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19: Interobserver Agreement Between Chest Radiologists.Can Assoc Radiol J. 2021 Feb;72(1):159-166. doi: 10.1177/0846537120938328. Epub 2020 Jul 2. Can Assoc Radiol J. 2021. PMID: 32615802 Free PMC article.
-
Radiological Society of North America Chest CT Classification System for Reporting COVID-19 Pneumonia: Interobserver Variability and Correlation with Reverse-Transcription Polymerase Chain Reaction.Radiol Cardiothorac Imaging. 2020 Jun 11;2(3):e200213. doi: 10.1148/ryct.2020200213. eCollection 2020 Jun. Radiol Cardiothorac Imaging. 2020. PMID: 33778589 Free PMC article.
-
RSNA and BSTI grading systems of COVID-19 pneumonia: comparison of the diagnostic performance and interobserver agreement.BMC Med Imaging. 2021 Oct 4;21(1):143. doi: 10.1186/s12880-021-00668-3. BMC Med Imaging. 2021. PMID: 34602051 Free PMC article.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Sep 30;9:CD013639. doi: 10.1002/14651858.CD013639.pub2. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. PMID: 32997361 Updated.
Cited by
-
Handheld Lung Ultrasound to Detect COVID-19 Pneumonia in Inpatients: A Prospective Cohort Study.POCUS J. 2023 Nov 27;8(2):175-183. doi: 10.24908/pocus.v8i2.16484. eCollection 2023. POCUS J. 2023. PMID: 38099168 Free PMC article.
-
Cascaded deep transfer learning on thoracic CT in COVID-19 patients treated with steroids.J Med Imaging (Bellingham). 2021 Jan;8(Suppl 1):014501. doi: 10.1117/1.JMI.8.S1.014501. Epub 2020 Dec 9. J Med Imaging (Bellingham). 2021. PMID: 33415179 Free PMC article.
-
Diagnostic prediction of COVID-19 based on clinical and radiological findings in a relatively low COVID-19 prevalence area.Respir Investig. 2021 Jul;59(4):446-453. doi: 10.1016/j.resinv.2021.03.002. Epub 2021 Mar 29. Respir Investig. 2021. PMID: 33865743 Free PMC article.
-
Diagnostic Performance of the Radiological Society of North America Consensus Statement for Reporting COVID-19 Chest CT Findings: A Revisit.J Clin Med. 2023 Aug 9;12(16):5180. doi: 10.3390/jcm12165180. J Clin Med. 2023. PMID: 37629222 Free PMC article.
-
Evaluation of the RSNA and CORADS classifications for COVID-19 on chest computed tomography in the Brazilian population.Clinics (Sao Paulo). 2021 Mar 26;76:e2476. doi: 10.6061/clinics/2021/e2476. eCollection 2021. Clinics (Sao Paulo). 2021. PMID: 33787655 Free PMC article.
References
-
- Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. American Journal of Roentgenology. American Roentgen Ray Society; 2020;1–7. - PubMed
LinkOut - more resources
Full Text Sources
