

Esophagopericardial Fistula Causing Pyopneumopericardium
- PMID: 33778644
- PMCID: PMC7977790
- DOI: 10.1148/ryct.2020200417
Esophagopericardial Fistula Causing Pyopneumopericardium
Abstract
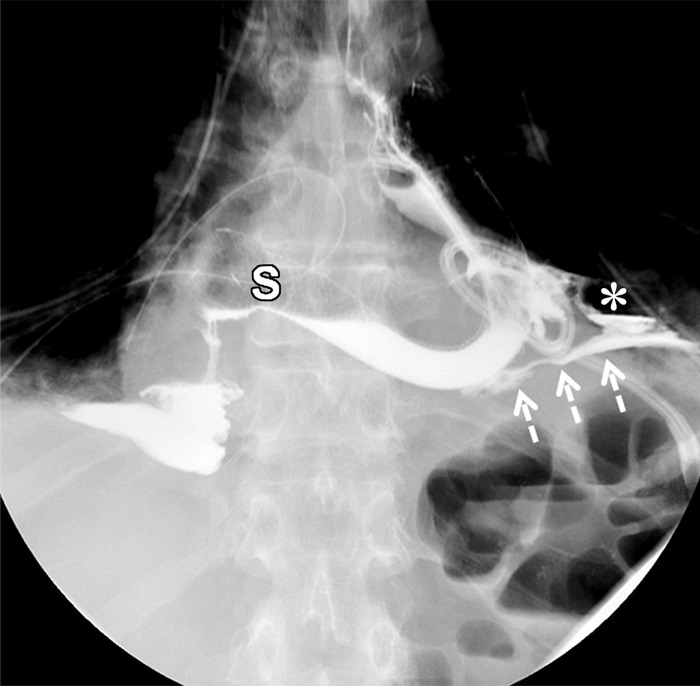
An esophagopericardial fistula is a rare complication of esophageal malignancy, trauma, or surgery. Imaging is a cornerstone of diagnosis, with detection of pneumopericardium or hydropneumopericardium at imaging raising suspicion for pyopneumopericardium and prompting immediate search for the causative pathologic process. Given the high associated mortality rate of over 50% for patients with esophagopericardial fistulas, early diagnosis and intervention are vital. Supplemental material is available for this article. © RSNA, 2020.
2020 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: A.W.B. disclosed no relevant relationships. D.J.D. disclosed no relevant relationships. R.T.F. disclosed no relevant relationships.
Figures




References
-
- Ladurner R, Qvick LM, Hohenbleicher F, Hallfeldt KK, Mutschler W, Mussack T. Pneumopericardium in blunt chest trauma after high-speed motor vehicle accidents. Am J Emerg Med 2005;23(1):83–86. - PubMed
-
- Farkas ZC, Pal S, Jolly GP, Lim MMD, Malik A, Malekan R. Esophagopericardial fistula and pneumopericardium from caustic ingestion and esophageal stent. Ann Thorac Surg 2019;107(3):e207–e208. - PubMed
-
- Dagres N, Kottkamp H, Piorkowski C, et al. Rapid detection and successful treatment of esophageal perforation after radiofrequency ablation of atrial fibrillation: lessons from five cases. J Cardiovasc Electrophysiol 2006;17(11):1213–1215. - PubMed
-
- Bunch TJ, Nelson J, Foley T, et al. Temporary esophageal stenting allows healing of esophageal perforations following atrial fibrillation ablation procedures. J Cardiovasc Electrophysiol 2006;17(4):435–439. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
