

Intratumoral Metabolic Heterogeneity and Other Quantitative 18F-FDG PET/CT Parameters for Prognosis Prediction in Esophageal Cancer
- PMID: 33778756
- PMCID: PMC7983774
- DOI: 10.1148/rycan.2020200022
Intratumoral Metabolic Heterogeneity and Other Quantitative 18F-FDG PET/CT Parameters for Prognosis Prediction in Esophageal Cancer
Abstract
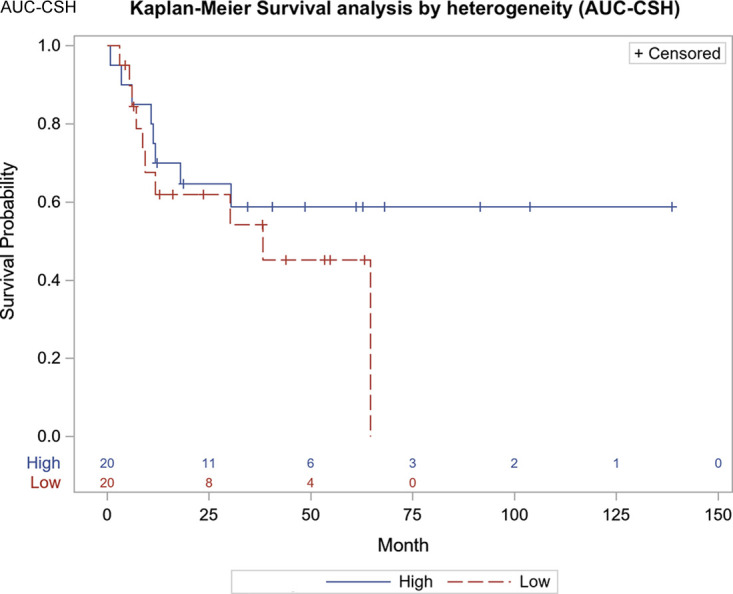
Purpose: To evaluate the impact of intratumoral metabolic heterogeneity (IMH) and other quantitative fluorine 18 (18F) fluorodeoxyglucose (FDG) PET/CT parameters for predicting progression-free survival (PFS) and overall survival (OS) in patients with esophageal cancer.
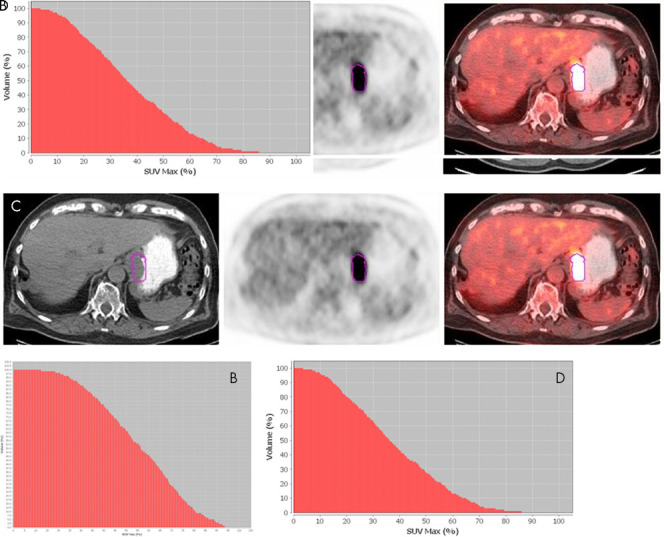
Materials and methods: In this retrospective study, an automated gradient-based segmentation method was used to assess the maximum standardized uptake value, mean standardized uptake value, metabolic tumor volume (MTV), and IMH index of the primary tumor in patients with biopsy-proven adenocarcinoma or squamous cell carcinoma of the esophagus with an initial staging 18F-FDG PET/CT. Data were collected between July 2006 and February 2016. OS and PFS were calculated using multivariable Cox proportional hazards regression with the adjustment (as covariates) of age, sex, weight, stage, tumor type, tumor grade, and treatment. All PET parameters were standardized before analysis. Log-rank tests were performed, and corresponding Kaplan-Meier survival plots were generated.
Results: A total of 71 patients (mean age, 64 years ± 10 [standard deviation], 62:9 men:women) were included. Median follow-up time was 28.2 months (range, 4-38 months), and median survival was 16.1 months (range, 0.1-60.3 months). Higher MTV was associated with reduced PFS for every standard deviation increase (hazard ratio [HR], 0.193; 95% CI: 0.052, 0.711; P = .01). Higher IMH was associated with reduced PFS for every standard deviation decrease in the area under the curve (HR, 10.78; 95% CI: 1.31, 88.96; P = .03).
Conclusion: PFS for patients with esophageal cancer was associated with MTV and with IMH.Keywords: Esophagus, Neoplasms-Primary, PET/CT, Tumor Response © RSNA, 2020.
2020 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: A.G. disclosed no relevant relationships. D.F.P. disclosed no relevant relationships. Y.X. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: employed by UT Southwestern Medical Center. Other relationships: disclosed no relevant relationships. R.S. disclosed no relevant relationships.
Figures
References
-
- Koshy M, Esiashvilli N, Landry JC, Thomas CR Jr, Matthews RH. Multiple management modalities in esophageal cancer: epidemiology, presentation and progression, work-up, and surgical approaches. Oncologist 2004;9(2):137–146. - PubMed
-
- Dong J, Thrift AP. Alcohol, smoking and risk of oesophago-gastric cancer. Best Pract Res Clin Gastroenterol 2017;31(5):509–517. - PubMed
-
- Engel LS, Chow WH, Vaughan TL, et al. Population attributable risks of esophageal and gastric cancers. J Natl Cancer Inst 2003;95(18):1404–1413. - PubMed
-
- Glenn TF. Esophageal cancer. Facts, figures, and screening. Gastroenterol Nurs 2001;24(6):271–273; quiz 274–275. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
