

Upgrade Rate of Pure Flat Epithelial Atypia Diagnosed at Core Needle Biopsy: A Systematic Review and Meta-Analysis
- PMID: 33778758
- PMCID: PMC7983762
- DOI: 10.1148/rycan.2021200116
Upgrade Rate of Pure Flat Epithelial Atypia Diagnosed at Core Needle Biopsy: A Systematic Review and Meta-Analysis
Abstract
Purpose: To perform a systematic review and meta-analysis to calculate the pooled upgrade rate of pure flat epithelial atypia (FEA) diagnosed at core needle biopsy (CNB).
Materials and methods: A PubMed and Embase database search was performed in December 2019. Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed. Study quality and publication bias were assessed. The upgrade rate of pure FEA to cancer, invasive carcinoma, and ductal carcinoma in situ (DCIS), as well as the co-occurrence rate of atypical ductal hyperplasia (ADH), with 95% CIs were calculated. A random effect model was used to integrate the proportions and their corresponding 95% CI. Study heterogeneity was calculated using τ2 and I 2 .
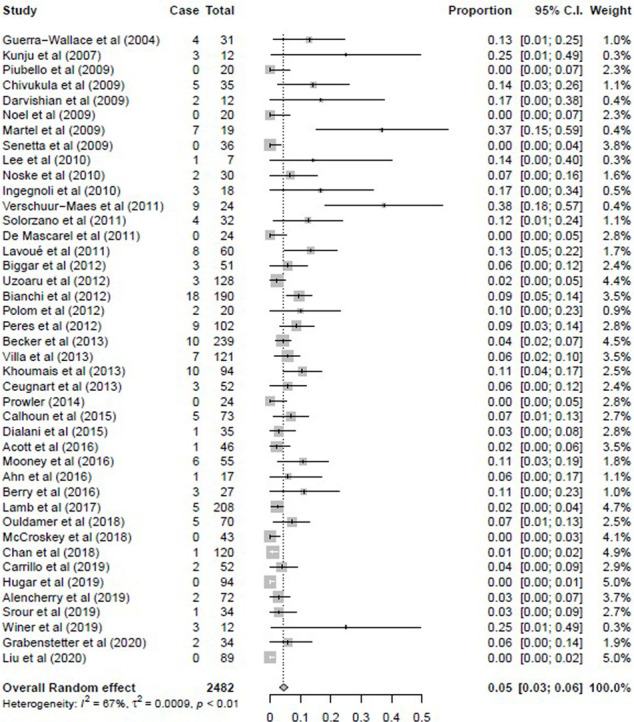
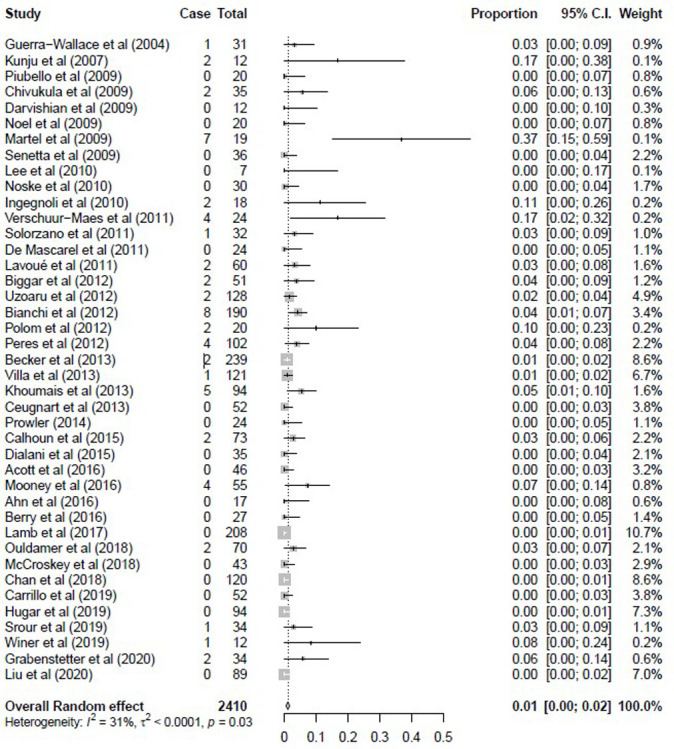
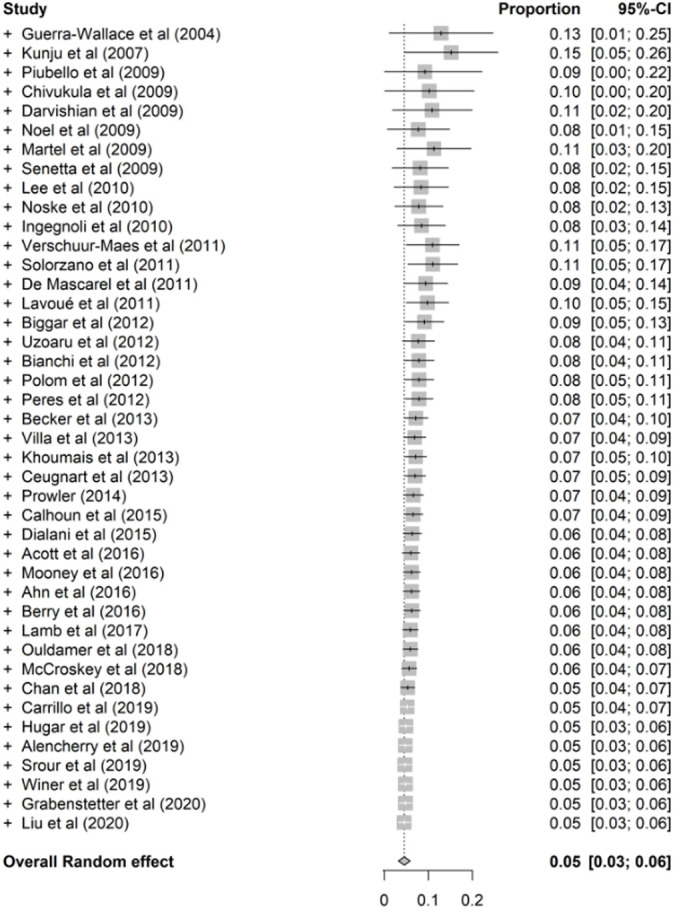
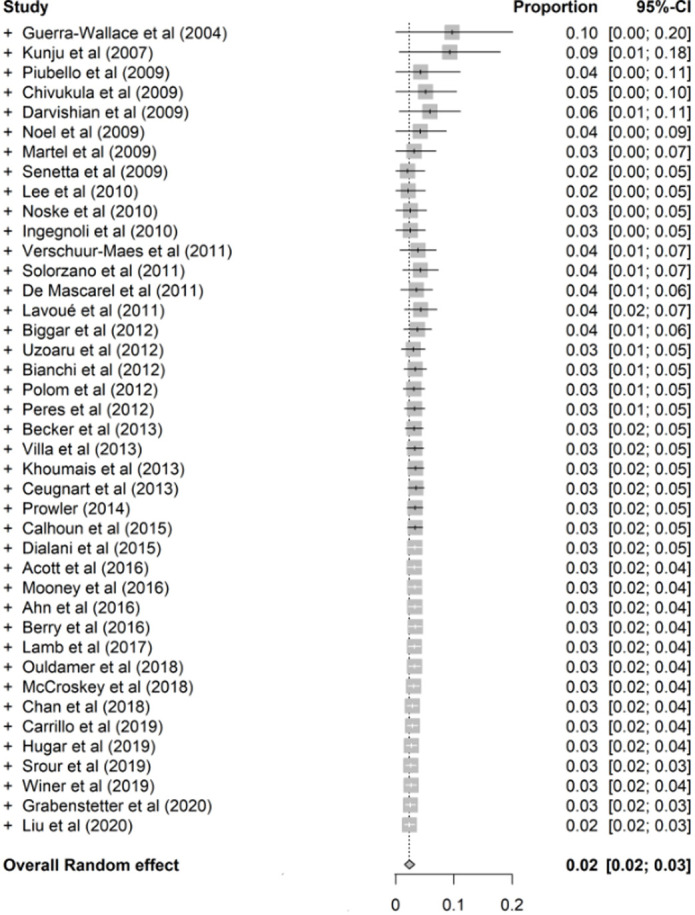
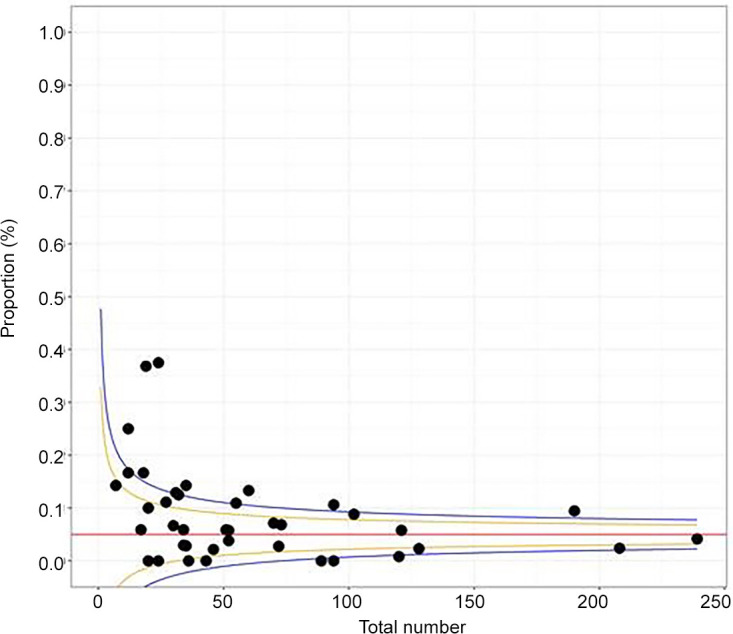
Results: A total of 2482 cases of pure FEA across 42 studies (mean age range, 46-59 years) met inclusion criteria to be analyzed. Significant study heterogeneity was identified (τ2 = 0.001, I 2 = 67%). The pooled upgrade rates reported for pure FEA were 5% (95% CI: 3%, 6%) for breast cancer, 1% (95% CI: 0%, 2%) for invasive carcinoma, and 2% (95% CI: 1%, 3%) for DCIS. When more than 90% of calcifications were removed at CNB, the pooled upgrade rate was 0% (95% CI: 0%, 2%). The pooled co-occurrence rate of ADH at surgical excision was 17% (95% CI: 12%, 21%). Study quality was medium to high with a risk of publication bias (P < .01).
Conclusion: Pure FEA diagnosed at CNB should be surgically excised due to the pooled upgrade rate of 5% for breast cancer. If more than 90% of the targeted calcifications are removed by CNB for pure FEA, close imaging follow-up is recommended.Keywords: Biopsy/Needle Aspiration, Breast, MammographySupplemental material is available for this article.© RSNA, 2021.
2021 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: R.A.W. disclosed no relevant relationships. S.J.L. disclosed no relevant relationships. M.EM. disclosed no relevant relationships. B.Z. disclosed no relevant relationships. M.C.M. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author is board member of the Radiological Society of North America and the American College of Radiology (ACR); author’s institution received Innovation Grant from ACR; author received royalties from Elsevier for breast textbook; author is editorial board member of Contemporary Diagnostic Radiology. Other relationships: disclosed no relevant relationships.
Figures





References
-
- Grabenstetter A, Brennan S, Salagean ED, Morrow M, Brogi E. Flat Epithelial Atypia in Breast Core Needle Biopsies With Radiologic-Pathologic Concordance: Is Excision Necessary? Am J Surg Pathol 2020;44(2):182–190.
-
- Rudin AV, Hoskin TL, Fahy A, et al. Flat Epithelial Atypia on Core Biopsy and Upgrade to Cancer: a Systematic Review and Meta-Analysis. Ann Surg Oncol 2017;24(12):3549–3558. - PubMed
-
- Acott AA, Mancino AT. Flat epithelial atypia on core needle biopsy, must we surgically excise? Am J Surg 2016;212(6):1211–1213. - PubMed
-
- Becker AK, Gordon PB, Harrison DA, et al. Flat ductal intraepithelial neoplasia 1A diagnosed at stereotactic core needle biopsy: is excisional biopsy indicated? AJR Am J Roentgenol 2013;200(3):682–688. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
