

Communicating Test Results from a General Health Check: Preferences from a Discrete Choice Experiment Survey
- PMID: 33778921
- PMCID: PMC8357669
- DOI: 10.1007/s40271-021-00512-4
Communicating Test Results from a General Health Check: Preferences from a Discrete Choice Experiment Survey
Abstract
Background: Health checks can detect risk factors and initiate prevention of cardiovascular diseases but there is no consensus on how to communicate the results. The aim of this study was to investigate the preferences of the general population for communicating health check results.
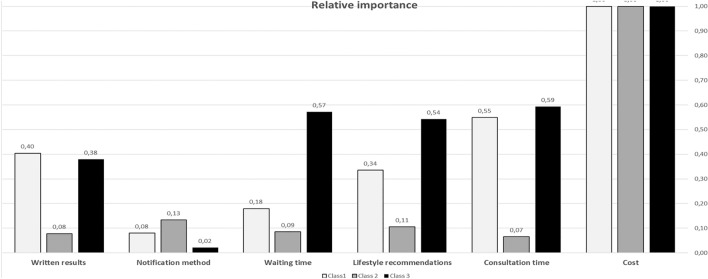
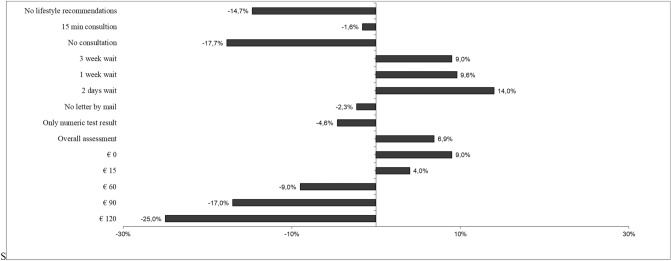
Methods: A randomly selected sample of the Swedish population aged 40-70 years completed a discrete choice experiment survey that included questions on sociodemographics, lifestyle and health and 15 choice questions consisting of six attributes (written results, notification method, consultation time, waiting time, lifestyle recommendation and cost). Data were analyzed with a latent class analysis (LCA). Relative importance of the attributes and predicted uptake for several scenarios were estimated.
Results: In the analysis, 432 individuals were included (response rate 29.6%). A three-class LCA model best fit the data. Cost was the most important attribute in all classes. Preferences heterogeneity was found for the other attributes; in Class 1, receiving consultation time and the written results were important, respondents in Class 2 dominated on costs and respondents in Class 3 found consultation time, waiting time and lifestyle recommendations to be important. Health literate respondents were more likely to belong to Class 3. The predicted uptake rates ranged from 7 to 88% for different health checks with large differences across the classes.
Conclusion: Cost was most important when deciding whether to participate in a health check. Although cost was the most important factor, it is not sufficient to offer health checks free-of-charge if other requirements regarding how the test results are communicated are not in place; participants need to be able to understand their results.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Piepoli MF, Hoes AW, Agewall S, Albus C, Brotons C, Catapano AL, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts): developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur J Prev Cardiol. 2016;23(11):np1–np96. 10.1177/2047487316653709. - PubMed
-
- Blomstedt Y, Norberg M, Stenlund H, Nyström L, Lönnberg G, Boman K, et al. Impact of a combined community and primary care prevention strategy on all-cause and cardiovascular mortality: a cohort analysis based on 1 million person-years of follow-up in Västerbotten County, Sweden, during 1990–2006. BMJ Open. 2015;5(12):e009651. doi: 10.1136/bmjopen-2015-009651. - DOI - PMC - PubMed
-
- WHO position paper on mammography screening. Geneva: World Health Organization; 2014. - PubMed
-
- Socialstyrelsen. Nationella screeningpreogram - modell för bedömning, införande och uppföljning: Socialstyrelsen. 2019.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
