

Assessment of Racial/Ethnic Disparities in Timeliness and Comprehensiveness of Dementia Diagnosis in California
- PMID: 33779684
- PMCID: PMC8008426
- DOI: 10.1001/jamaneurol.2021.0399
Assessment of Racial/Ethnic Disparities in Timeliness and Comprehensiveness of Dementia Diagnosis in California
Abstract
Importance: The US aging population is rapidly becoming more racially and ethnically diverse. Early diagnosis of dementia is a health care priority.
Objective: To examine the associations between race/ethnicity and timeliness of dementia diagnosis and comprehensiveness of diagnostic evaluation.
Design, setting, and participants: This retrospective cross-sectional study used 2013-2015 California Medicare fee-for-service data to examine the associations of race/ethnicity, individual factors, and contextual factors with the timeliness and comprehensiveness of dementia diagnosis. Data from 10 472 unique beneficiaries were analyzed. The sample was selected on the basis of the following criteria: presence of 1 or more claims; no diagnoses of dementia or mild cognitive impairment in 2013 to 2014; continuous enrollment in Medicare Parts A and B; Asian, Black, Hispanic, or White race/ethnicity; and incident diagnoses of dementia or mild cognitive impairment in January through June 2015. Data analyses were conducted from November 1, 2019, through November 10, 2020.
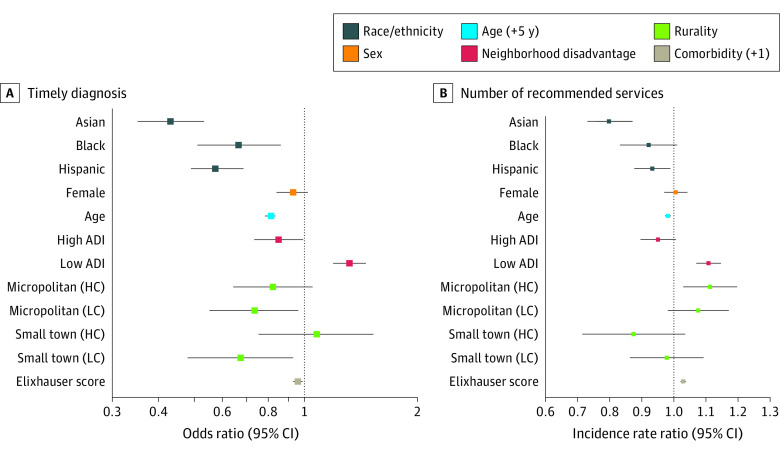
Main outcomes and measures: Timeliness of diagnosis, defined as incident diagnosis of mild cognitive impairment vs dementia, and comprehensiveness of diagnostic evaluation, defined as presence of the following services in claims within 6 months before or after the incident diagnosis date: specialist evaluation, laboratory testing, and neuroimaging studies.
Results: The sample comprised 10 472 unique Medicare beneficiaries with incident diagnoses of dementia or mild cognitive impairment (6504 women [62.1%]; mean [SD] age, 82.9 [8.0] years) and included 993 individuals who identified as Asian (9.5%), 407 as Black (3.9%), 1255 as Hispanic (12.0%), and 7817 as White (74.6%). Compared with White beneficiaries, those who identified as Asian (odds ratio, 0.46; 95% CI, 0.38-0.56), Black (odds ratio, 0.73; 95% CI, 0.56-0.94), or Hispanic (odds ratio, 0.62; 95% CI, 0.52-0.72) were less likely to receive a timely diagnosis. Asian beneficiaries (incidence rate ratio, 0.81; 95% CI, 0.74-0.87) also received fewer diagnostic evaluation elements. These associations remained significant after adjusting for age, sex, comorbidity burden, neighborhood disadvantage, and rurality.
Conclusions and relevance: These findings highlight substantial disparities in the timeliness and comprehensiveness of dementia diagnosis. Public health interventions are needed to achieve equitable care for people living with dementia across all racial/ethnic groups.
Conflict of interest statement
Figures
Comment in
-
Diversity and Disparities in Dementia Diagnosis and Care: A Challenge for All of Us.JAMA Neurol. 2021 Jun 1;78(6):650-652. doi: 10.1001/jamaneurol.2021.0285. JAMA Neurol. 2021. PMID: 33779687 No abstract available.
References
-
- World Health Organization. Dementia: a public health priority. Published 2012. Accessed June 30, 2020. https://www.who.int/mental_health/publications/dementia_report_2012/en/
-
- Alzheimer’s Disease International. World Alzheimer report 2015: the global impact of dementia: an analysis of prevalence, incidence, cost and trends. Updated October 2015. Accessed June 30, 2020. https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf
-
- Alzheimer’s Association. 2020 Alzheimer’s disease facts and figures. Accessed June 30, 2020. https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf
-
- US Department of Health and Human Services. National plan to address Alzheimer’s disease: 2019 update. Accessed August 12, 2020. https://aspe.hhs.gov/system/files/pdf/262601/NatlPlan2019.pdf
-
- Schneider J, Jeon S, Gladman JT, Corriveau RA, 2019. ADRD Summit 2019 report to the National Advisory Neurological Disorders and Stroke Council. Published September 4, 2019. Accessed August 12, 2020. https://www.ninds.nih.gov/sites/default/files/2019_adrd_summit_recommend...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
