

Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis
- PMID: 33779745
- PMCID: PMC8008284
- DOI: 10.1001/jamanetworkopen.2021.3520
Association of Obesity With Survival Outcomes in Patients With Cancer: A Systematic Review and Meta-analysis
Abstract
Importance: Obesity, defined as a body mass index (BMI) greater than 30, is associated with a significant increase in the risk of many cancers and in overall mortality. However, various studies have suggested that patients with cancer and no obesity (ie, BMI 20-25) have worse outcomes than patients with obesity.
Objective: To assess the association between obesity and outcomes after a diagnosis of cancer.
Data sources: PubMed, the Cochrane Library, and EMBASE were searched from inception to January 2020.
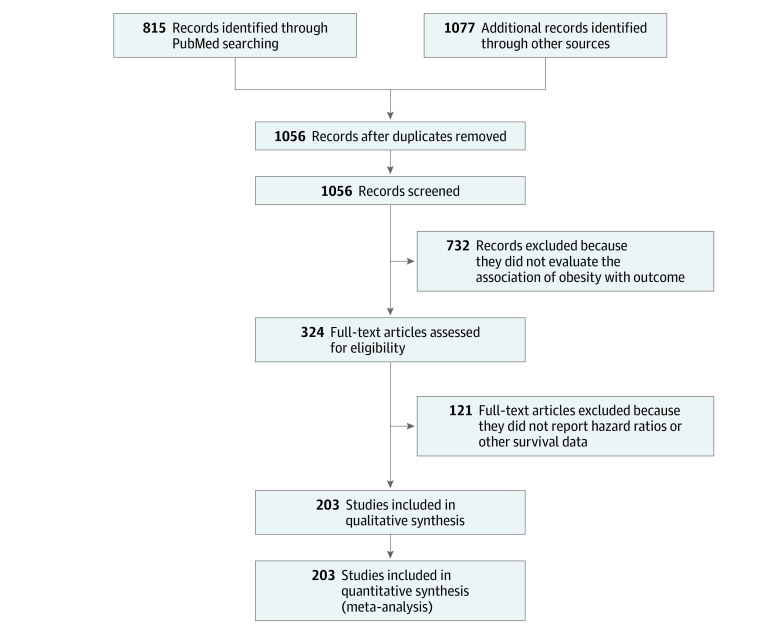
Study selection: Studies reporting prognosis of patients with obesity using standard BMI categories and cancer were included. Studies that used nonstandard BMI categories, that were limited to children, or that were limited to patients with hematological malignant neoplasms were excluded. Screening was performed independently by multiple reviewers. Among 1892 retrieved studies, 203 (17%) met inclusion criteria for initial evaluation.
Data extraction and synthesis: The Meta-analysis of Observational Studies in Epidemiology (MOOSE) and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) reporting guidelines were reporting guideline was followed. Data were extracted by multiple independent reviewers. Risk of death, cancer-specific mortality, and recurrence were pooled to provide an adjusted hazard ratio (HR) with a 95% CI . A random-effects model was used for the retrospective nature of studies.
Main outcomes and measures: The primary outcome of the study was overall survival (OS) in patients with cancer, with and without obesity. Secondary end points were cancer-specific survival (CSS) and progression-free survival (PFS) or disease-free survival (DFS). The risk of events was reported as HRs with 95% CIs, with an HR greater than 1 associated with a worse outcome among patients with obesity vs those without.
Results: A total of 203 studies with 6 320 365 participants evaluated the association of OS, CSS, and/or PFS or DFS with obesity in patients with cancer. Overall, obesity was associated with a reduced OS (HR, 1.14; 95% CI, 1.09-1.19; P < .001) and CSS (HR, 1.17; 95% CI, 1.12-1.23; P < .001). Patients were also at increased risk of recurrence (HR, 1.13; 95% CI, 1.07-1.19; P < .001). Conversely, patients with obesity and lung cancer, renal cell carcinoma, or melanoma had better survival outcomes compared with patients without obesity and the same cancer (lung: HR, 0.86; 95% CI, 0.76-0.98; P = .02; renal cell: HR, 0.74; 95% CI, 0.53-0.89; P = .02; melanoma: HR, 0.74; 95% CI, 0.57-0.96; P < .001).
Conclusions and relevance: In this study, obesity was associated with greater mortality overall in patients with cancer. However, patients with obesity and lung cancer, renal cell carcinoma, and melanoma had a lower risk of death than patients with the same cancers without obesity. Weight-reducing strategies may represent effective measures for reducing mortality in these patients.
Conflict of interest statement
References
-
- World Health Organization. Obesity: Preventing and Managing the Global Epidemic. World Health Organization; 2000. Accessed February 24, 2021. https://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
