

Utility of Fetal Cardiovascular Magnetic Resonance for Prenatal Diagnosis of Complex Congenital Heart Defects
- PMID: 33779747
- PMCID: PMC8008290
- DOI: 10.1001/jamanetworkopen.2021.3538
Utility of Fetal Cardiovascular Magnetic Resonance for Prenatal Diagnosis of Complex Congenital Heart Defects
Erratum in
-
Errors in Figure Titles and Article Information.JAMA Netw Open. 2021 Apr 1;4(4):e2111261. doi: 10.1001/jamanetworkopen.2021.11261. JAMA Netw Open. 2021. PMID: 33890998 Free PMC article. No abstract available.
-
Author Name Change.JAMA Netw Open. 2022 Mar 1;5(3):e225825. doi: 10.1001/jamanetworkopen.2022.5825. JAMA Netw Open. 2022. PMID: 35289868 Free PMC article. No abstract available.
Abstract
Importance: Prenatal diagnosis of complex congenital heart defects reduces mortality and morbidity in affected infants. However, fetal echocardiography can be limited by poor acoustic windows, and there is a need for improved diagnostic methods.
Objective: To assess the clinical utility of fetal cardiovascular magnetic resonance imaging in cases in which fetal echocardiography could not visualize all relevant anatomy.
Design, setting, and participants: This cohort study was conducted between January 20, 2017, and June 29, 2020, at Skåne University Hospital (Lund, Sweden), a tertiary center for pediatric cardiology and thoracic surgery. Participants were fetuses referred for fetal cardiovascular magnetic resonance examination by a pediatric cardiologist after an inconclusive echocardiograph.
Exposures: Fetal cardiovascular magnetic resonance examination requested by the patient's pediatric cardiologist.
Main outcomes and measures: Any change in patient management because of diagnostic information gained from fetal cardiovascular magnetic resonance imaging.
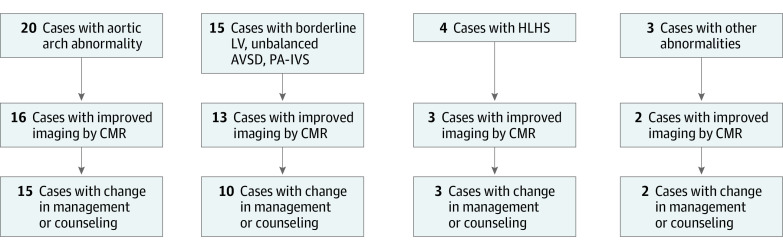
Results: A total of 31 fetuses underwent cardiovascular magnetic resonance examination at a median gestational age of 36 weeks (range, 31-39 weeks). Overall, fetal cardiovascular magnetic resonance imaging had clinical utility, affecting patient management and/or parental counseling in 26 cases (84%). For aortic arch anatomy including signs of coarctation (20 fetuses), fetal cardiovascular magnetic resonance imaging added diagnostic information in 16 cases (80%). For assessment of univentricular vs biventricular outcome in borderline left ventricle, unbalanced atrioventricular septal defect, and pulmonary atresia with intact ventricular septum (15 fetuses), fetal cardiovascular magnetic resonance imaging visualized intracardiac anatomy and ventricular function, allowing assessment of outcome in 13 cases (87%). In 4 fetuses with hypoplastic left heart syndrome, fetal cardiovascular magnetic resonance imaging helped delivery planning in 3 cases (75%). Finally, fetal cardiovascular magnetic resonance imaging provided valuable information for parental counseling in 21 cases (68%).
Conclusions and relevance: In this cohort study, fetal cardiovascular magnetic resonance imaging added clinically useful information to what was available from echocardiography. These findings suggest that fetal CMR has the potential to affect clinical decision-making in challenging cases of congenital heart defects with inconclusive data from echocardiography. Fetal cardiovascular magnetic resonance imaging showed an association with clinical decision-making, including mode of delivery and early postnatal care, as well as with parental counseling.
Conflict of interest statement
Figures
Comment in
-
Fetal Cardiac Imaging for Congenital Heart Disease-Is Cardiac Magnetic Resonance Imaging the Future?JAMA Netw Open. 2021 Mar 1;4(3):e214617. doi: 10.1001/jamanetworkopen.2021.4617. JAMA Netw Open. 2021. PMID: 33779739 No abstract available.
References
-
- Satomi G, Yasukochi S, Shimizu T, Takigiku K, Ishii T. Has fetal echocardiography improved the prognosis of congenital heart disease? comparison of patients with hypoplastic left heart syndrome with and without prenatal diagnosis. Pediatr Int. 1999;41(6):728-732. doi: 10.1046/j.1442-200x.1999.01154.x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
