

Radioembolization versus portal vein embolization for contralateral liver lobe hypertrophy: effect of cirrhosis
- PMID: 33779787
- PMCID: PMC8286933
- DOI: 10.1007/s00261-021-03048-1
Radioembolization versus portal vein embolization for contralateral liver lobe hypertrophy: effect of cirrhosis
Abstract
Purpose: Preoperative hypertrophy induction of future liver remnant (FLR) reduces the risk of postoperative liver insufficiency after partial hepatectomy. One of the most commonly used methods to induce hypertrophy of FLR is portal vein embolization (PVE). Recent studies have shown that transarterial radioembolization (TARE) also induces hypertrophy of the contralateral liver lobe. The aim of our study was to evaluate contralateral hypertrophy after TARE versus after PVE taking into account the effect of cirrhosis.
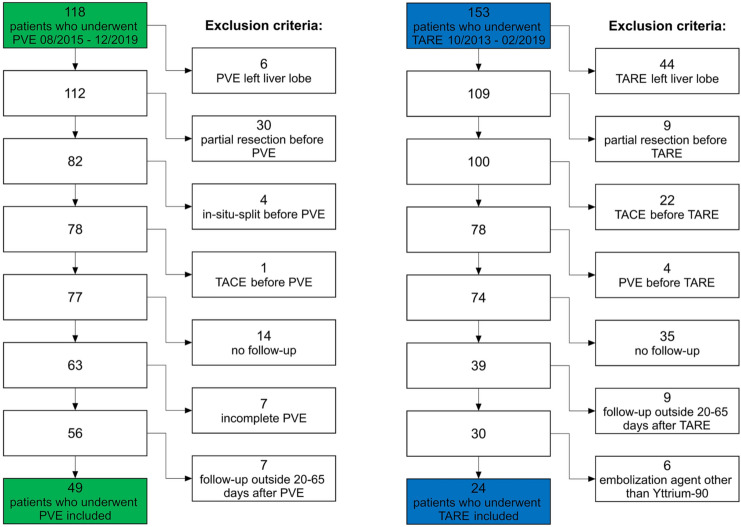
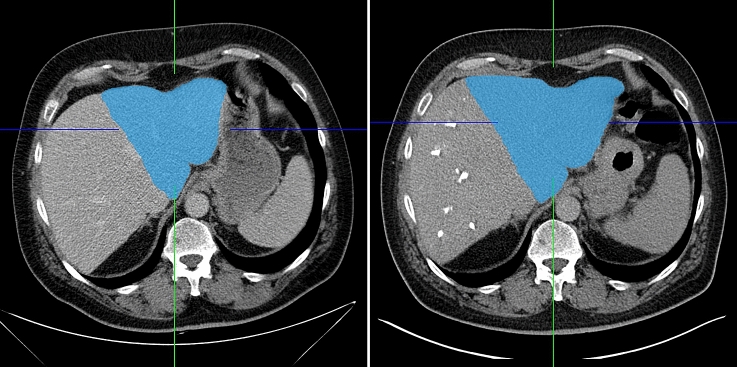
Methods: Forty-nine patients undergoing PVE before hemihepatectomy and 24 patients with TARE as palliative treatment for liver malignancy were retrospectively included. Semi-automated volumetry of the FLR/contralateral liver lobe before and after intervention (20 to 65 days) was performed on CT or MRI, and the relative increase in volume was calculated. Cirrhosis was evaluated independently by two radiologists on CT/MRI, and interrater reliability was calculated.
Results: Hypertrophy after PVE was significantly more pronounced than after TARE (25.3% vs. 7.4%; p < 0.001). In the subgroup of patients without cirrhosis, the difference was also statistically significant (25.9% vs. 8.6%; p = 0.002), whereas in patients with cirrhosis, the difference was not statistically significant (18.2% vs. 7.4%; p = 0.212). After PVE, hypertrophy in patients without cirrhosis was more pronounced than in patients with cirrhosis (25.9% vs. 18.2%; p = 0.203), while after TARE, hypertrophy was comparable in patients with and without cirrhosis (7.4% vs. 8.6%; p = 0.928).
Conclusion: TARE induces less pronounced hypertrophy of the FLR compared to PVE. Cirrhosis seems to be less of a limiting factor for hypertrophy after TARE, compared to PVE.
Keywords: Hepatic artery; Hypertrophy; Liver cirrhosis; Portal vein; Therapeutic embolization.
© 2021. The Author(s).
Figures



Similar articles
-
Induction of Contralateral Hepatic Hypertrophy by Unilobar Yttrium-90 Transarterial Radioembolization versus Portal Vein Embolization: An Animal Study.J Vasc Interv Radiol. 2021 Jun;32(6):836-842.e2. doi: 10.1016/j.jvir.2021.01.281. Epub 2021 Mar 6. J Vasc Interv Radiol. 2021. PMID: 33689835
-
Sequential Y90 liver radioembolization and portal vein embolization: an additional strategy to downstage liver tumors and to enhance liver hypertrophy before major hepatectomies.Langenbecks Arch Surg. 2023 Aug 28;408(1):339. doi: 10.1007/s00423-023-03083-0. Langenbecks Arch Surg. 2023. PMID: 37639197
-
Hepatic vein embolization after portal vein embolization to induce additional liver hypertrophy in patients with metastatic colorectal carcinoma.Eur Radiol. 2020 Jul;30(7):3862-3868. doi: 10.1007/s00330-020-06746-4. Epub 2020 Mar 7. Eur Radiol. 2020. PMID: 32144462
-
Portal Vein Embolization Utilizing N-Butyl Cyanoacrylate for Contralateral Lobe Hypertrophy Prior to Liver Resection: A Systematic Review and Meta-Analysis.Cardiovasc Intervent Radiol. 2018 Sep;41(9):1302-1312. doi: 10.1007/s00270-018-1964-6. Epub 2018 Apr 23. Cardiovasc Intervent Radiol. 2018. PMID: 29687262
-
Transarterial Radioembolization to Impact Liver Volumetry: When and How.Cardiovasc Intervent Radiol. 2022 Nov;45(11):1646-1650. doi: 10.1007/s00270-022-03218-8. Epub 2022 Jul 20. Cardiovasc Intervent Radiol. 2022. PMID: 35859212 Review.
Cited by
-
Augmenting the Future Liver Remnant Prior to Major Hepatectomy: A Review of Options on the Menu.Ann Surg Oncol. 2025 Aug;32(8):5694-5709. doi: 10.1245/s10434-025-17607-z. Epub 2025 Jun 8. Ann Surg Oncol. 2025. PMID: 40483651 Free PMC article. Review.
-
Interventional radiological therapies in colorectal hepatic metastases.Front Oncol. 2023 May 30;13:963966. doi: 10.3389/fonc.2023.963966. eCollection 2023. Front Oncol. 2023. PMID: 37324012 Free PMC article. Review.
-
Initial experience with Double-vein Embolization in Hungary.Eur J Radiol Open. 2024 Nov 21;13:100613. doi: 10.1016/j.ejro.2024.100613. eCollection 2024 Dec. Eur J Radiol Open. 2024. PMID: 39639858 Free PMC article.
-
Hepatobiliary scintigraphy and liver function changes in patients with hepatocellular carcinoma treated with 166Ho-radioembolization : HBS in HCC treated with holmium-166.EJNMMI Res. 2025 Jan 9;15(1):2. doi: 10.1186/s13550-025-01196-9. EJNMMI Res. 2025. PMID: 39786516 Free PMC article.
References
-
- Capussotti L, Muratore A, Baracchi F, et al (2008) Portal vein ligation as an efficient method of increasing the future liver remnant volume in the surgical treatment of colorectal metastases. Arch Surg Chic Ill 1960 143:978–982; discussion 982. 10.1001/archsurg.143.10.978 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
