

Clinical performance of lung ultrasound in predicting ARDS morphology
- PMID: 33779834
- PMCID: PMC8006629
- DOI: 10.1186/s13613-021-00837-1
Clinical performance of lung ultrasound in predicting ARDS morphology
Abstract
Background: To assess diagnostic performance of lung ultrasound (LUS) in identifying ARDS morphology (focal vs non-focal), compared with the gold standard computed tomography.
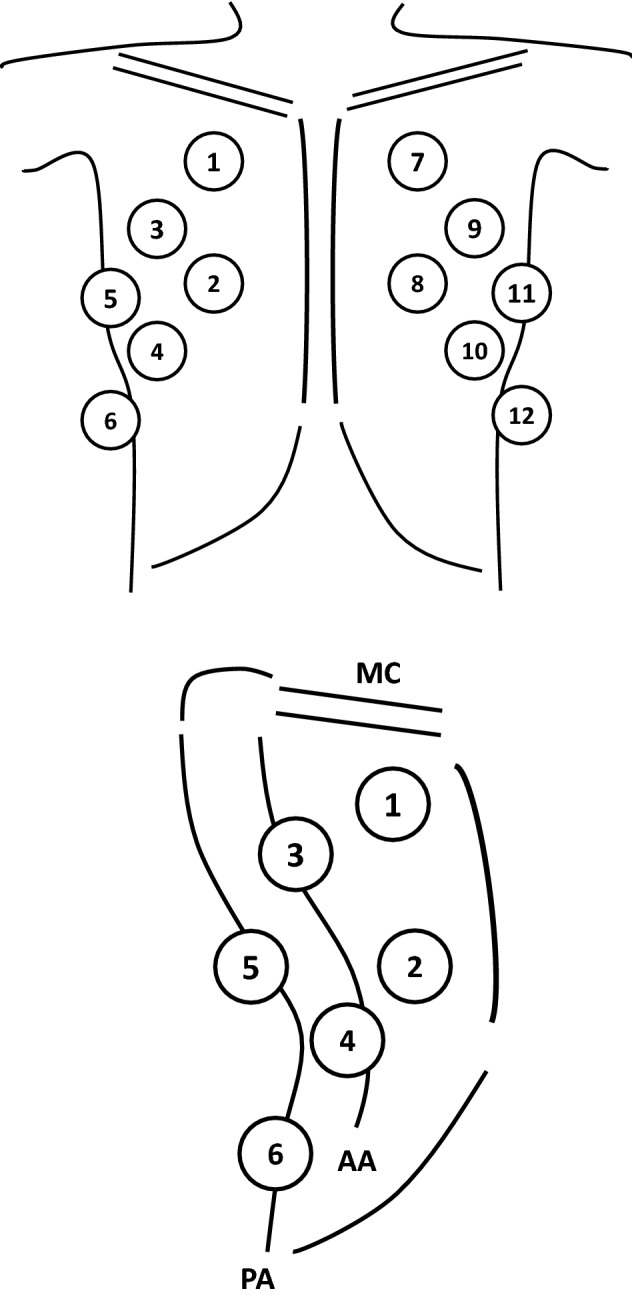
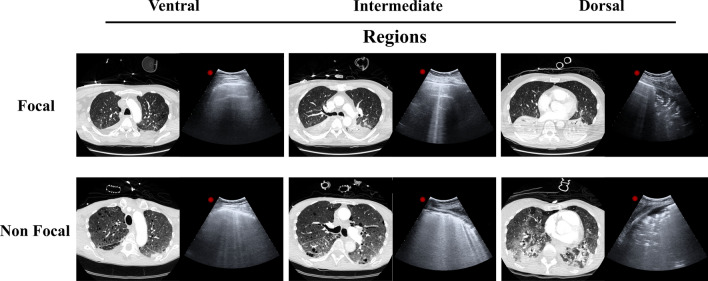
Methods: Mechanically ventilated ARDS patients undergoing lung computed tomography and ultrasound were enrolled. Twelve fields, were evaluated. LUS score was graded from 0 (normal) to 3 (consolidation) according to B-lines extent. Total and regional LUS score as the sum of the four ventral (LUSV), intermediate (LUSI) or dorsal (LUSD) fields, were calculated. Based on lung CT, ARDS morphology was defined as (1) focal (loss of aeration with lobar distribution); (2) non-focal (widespread loss of aeration or segmental loss of aeration distribution associated with uneven lung attenuation areas), and diagnostic accuracy of LUS in discriminating ARDS morphology was determined by AU-ROC in training and validation set of patients.
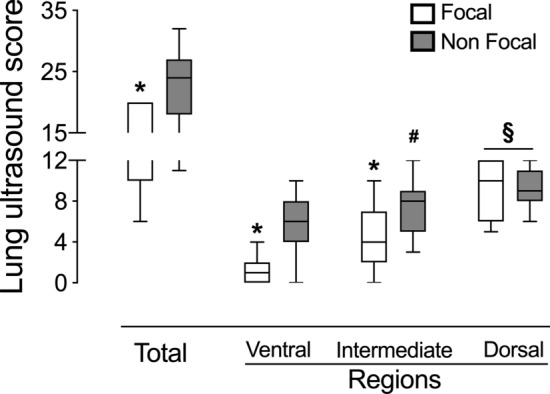
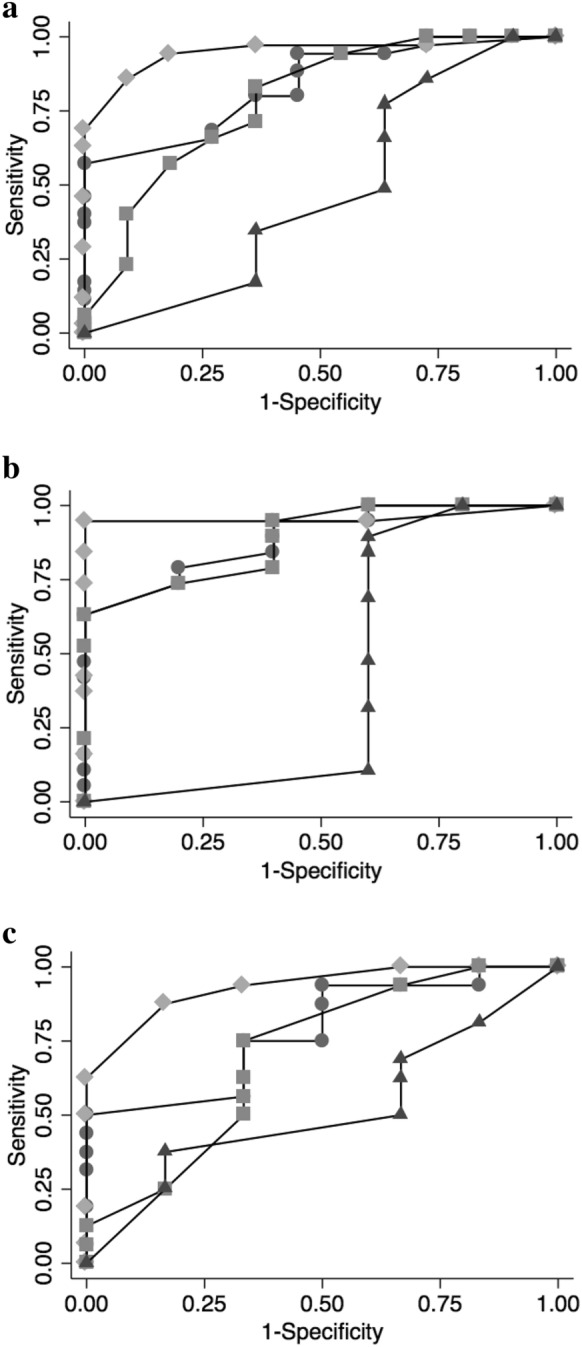
Results: Forty-seven patients with ARDS (25 training set and 22 validation set) were enrolled. LUSTOT, LUSV and LUSI but not LUSD score were significantly lower in focal than in non-focal ARDS morphologies (p < .01). The AU-ROC curve of LUSTOT, LUSV, LUSI and LUSD for identification of non-focal ARDS morphology were 0.890, 0.958, 0.884 and 0.421, respectively. LUSV value ≥ 3 had the best predictive value (sensitivity = 0.95, specificity = 1.00) in identifying non-focal ARDS morphology. In the validation set, an LUSV score ≥ 3 confirmed to be highly predictive of non-focal ARDS morphology, with a sensitivity and a specificity of 94% and 100%.
Conclusions: LUS had a valuable performance in distinguishing ARDS morphology.
Keywords: ARDS; ARDS morphology; Bedside tests; Lung ultrasound; Point of care diagnostic tests; Respiratory monitoring.
Conflict of interest statement
The authors report the absence of conflicts of interest related to the submitted work.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
