

Maximum bite force in children with juvenile idiopathic arthritis with and without clinical established temporomandibular joint involvement and in healthy children: a cross-sectional study
- PMID: 33780558
- PMCID: PMC8251949
- DOI: 10.1111/joor.13172
Maximum bite force in children with juvenile idiopathic arthritis with and without clinical established temporomandibular joint involvement and in healthy children: a cross-sectional study
Abstract
Background: In children with juvenile idiopathic arthritis (JIA), the temporomandibular joint (TMJ) can be involved, resulting in dysfunction of the masticatory system. Bite force is one of the variables that reflects the function of the masticatory system. The aim of this study was to compare maximum bite force in children with JIA, with and without TMJ involvement and with healthy children.
Methods: Children with JIA and healthy children between the ages 6 and 18 were included in this cross-sectional study. The clinical examination consisted of measuring the anterior maximum voluntary bite force (AMVBF), assessment of the TMJ screening protocol items and TMJ, masseter and temporal muscle palpation pain. Unadjusted linear regression analyses were performed to evaluate the explanatory factors for AMVBF. Two adjusted models were constructed with corrections for age and gender differences: model 1 to compare children with JIA and healthy children and model 2 to compare children with JIA with and without TMJ involvement.
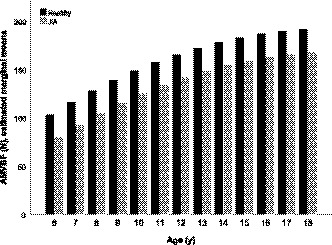
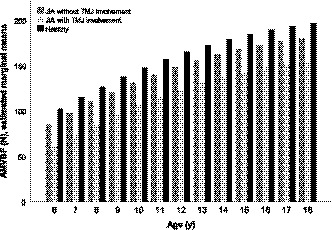
Results: In this cross-sectional study, 298 children with JIA and 169 healthy children participated. AMVBF was 24 Newton (N) lower in children with JIA, when compared with healthy children (95%CI: -35.5--12.4, p = .000). When children with JIA also had clinically established TMJ involvement, AMVBF was reduced 42 N (component JIA:-16.78, 95% CI -28.96--4.59, p = .007 and component TMJ involvement:-25.36, 95% CI -40.08--10.63, p = .001). Age and male gender increased AMVBF.
Conclusion: Children with JIA had a reduction in the AMVBF compared with healthy children. In children with JIA and clinically established TMJ involvement, AMVBF was more reduced.
Keywords: arthritis; bite force; child; cross-sectional studies; juvenile; linear models; temporomandibular joint.
© 2021 John Wiley & Sons Ltd.
Conflict of interest statement
The authors report no financial conflicts of interest.
Figures
References
-
- Petty RE, Southwood TR, Manners P, et al. International league of associations for rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004;31(2):390‐392. - PubMed
-
- Kellenberger CJ, Junhasavasdikul T, Tolend M, Doria AS, Kellenberger CJ. Identification and grading of juvenile idiopathic arthritis related changes in the temporomandibular joints in contrast enhanced magnetic resonance imaging: an imaging atlas. Pediatr Radiol. 2017;47(S1):1‐296. 10.1007/s00247-017-3809-x - DOI
-
- Arabshahi B, Cron RQ. Temporomandibular joint arthritis in juvenile idiopathic arthritis: the forgotten joint. Curr Opin Rheumatol. 2006;18:490‐495. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
