

Is double-strut fibula ankle arthrodesis a reliable reconstruction for bone defect after distal tibia tumor resection?-a finite element study based on promising clinical outcomes
- PMID: 33781282
- PMCID: PMC8006370
- DOI: 10.1186/s13018-021-02362-0
Is double-strut fibula ankle arthrodesis a reliable reconstruction for bone defect after distal tibia tumor resection?-a finite element study based on promising clinical outcomes
Abstract
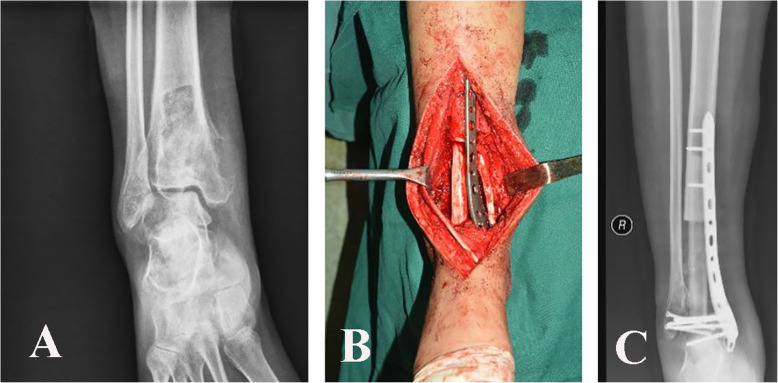
Background: There are different surgical methods for primary malignant tumor located at distal tibia. Previous studies have reported that double-strut fibula ankle arthrodesis is an alternative option. The purpose of this study was to investigate the biomechanical effect of double-strut fibula ankle arthrodesis by finite element analysis (FEA).
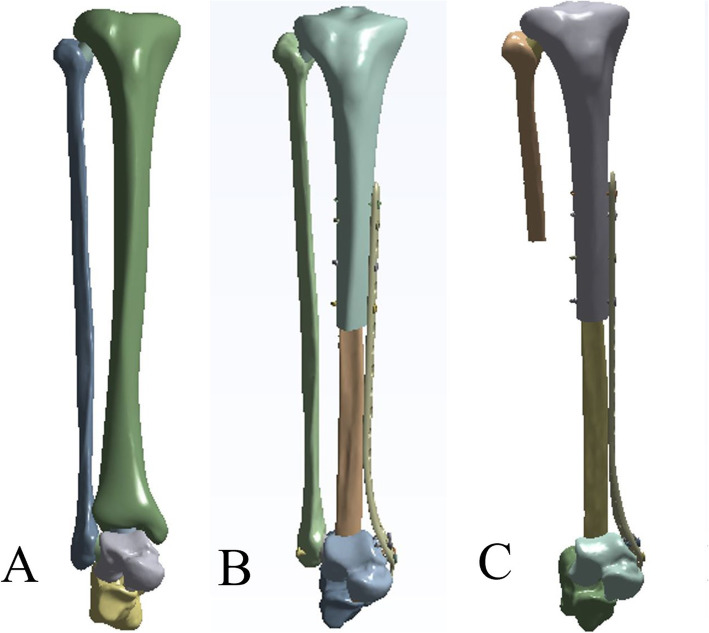
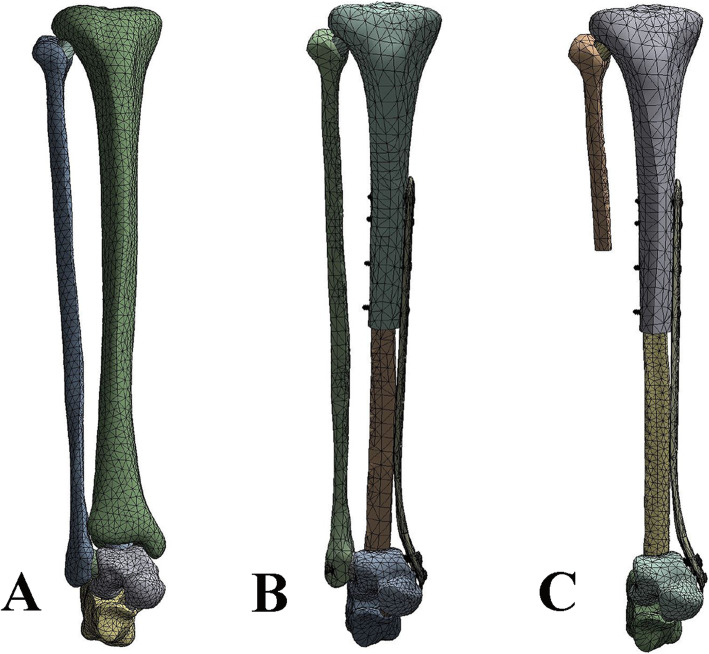
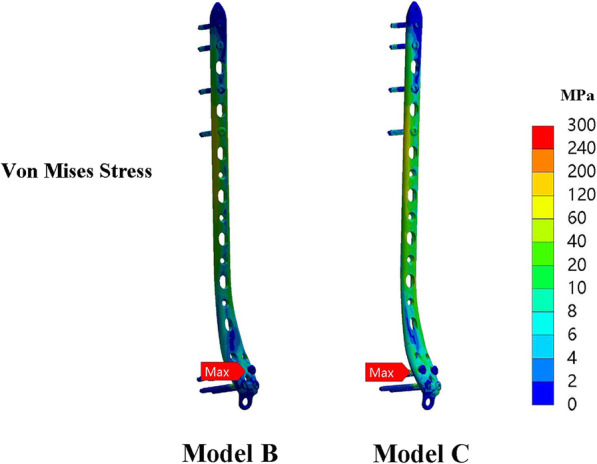
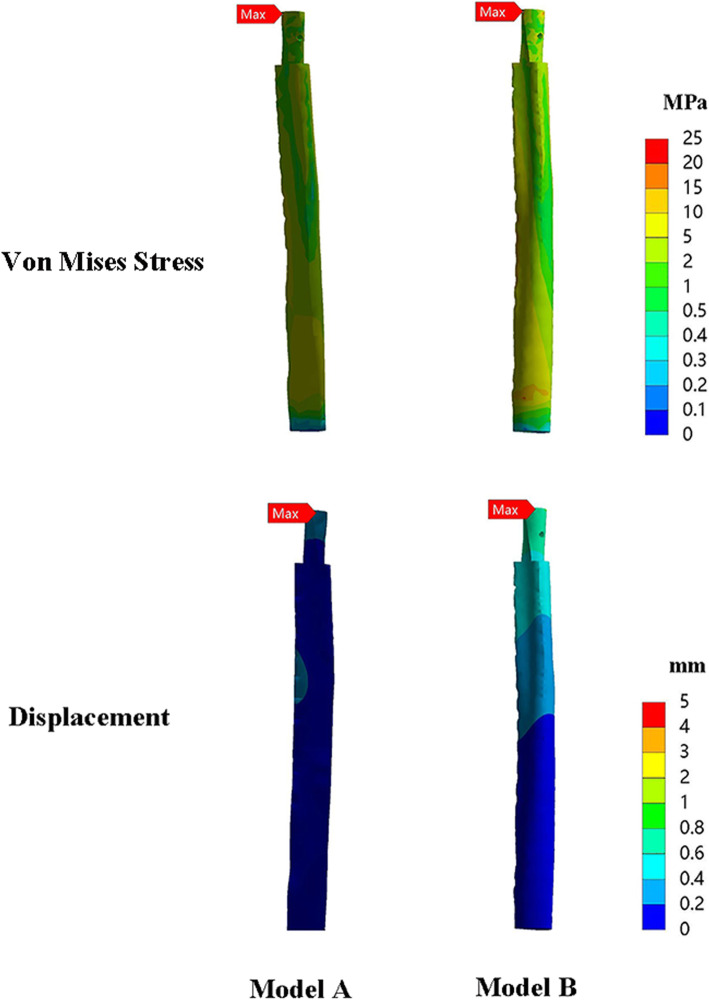
Methods: Computer-aided design software was used to establish three-dimension models. Three different models were constructed: normal tibia-fibula-talus complex (model A), double-strut fibula ankle arthrodesis (model B), and reconstruction by ipsilateral fibula (model C). We used FEA to evaluate and compare the biomechanical characteristics of these constructs. Simulated load of 600 N was applied to the tibial plateau to simulate balanced single-foot standing. Output results representing the model von Mises stress and displacement of the components were analyzed.
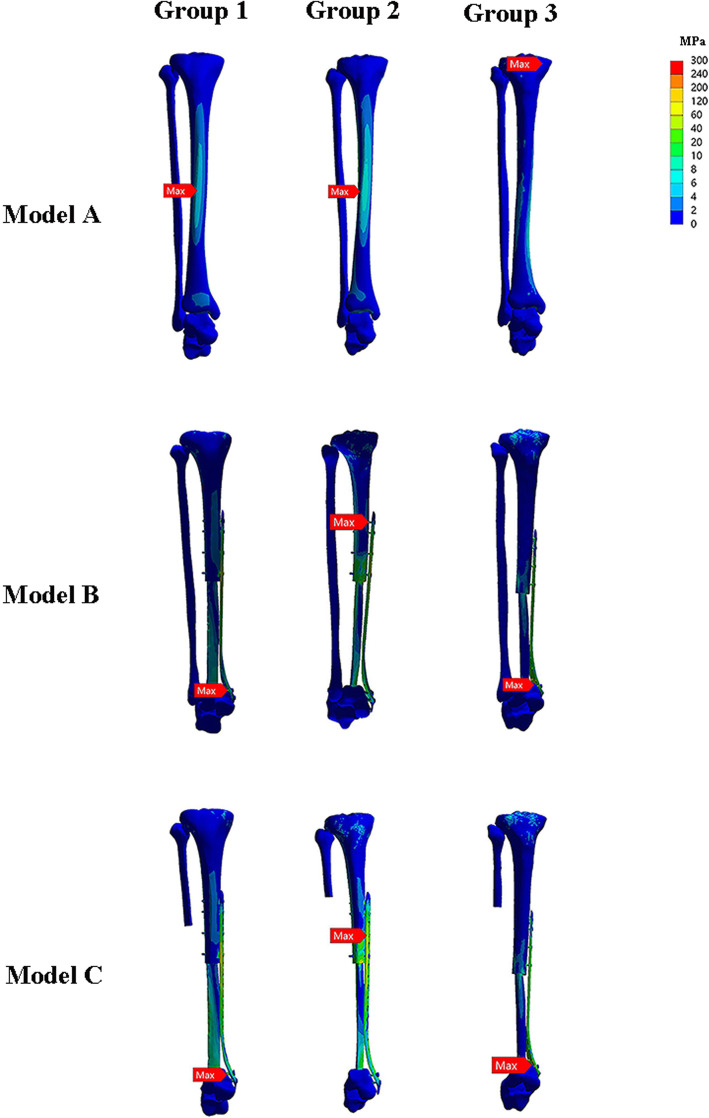
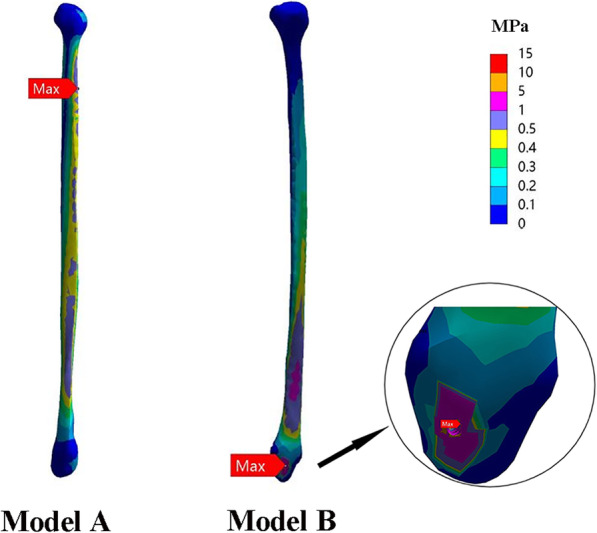
Results: Construct stiffness was increased when the internal plate fixation was used. For axial load, model B (1460.5 N/mm) was stiffer than the construct of model A (524.8 N/mm), and model C (636.6 N/mm), indicating model B was more stable. Maximum stress on the fibular graft occurred on the proximal end. The von Mises stress and stress distribution of fibular graft in model B (71.4 MPa) and model C (67.8 MPa) were similar. In model B, the ipsilateral fibula in model B has a higher value of stress (16.1 MPa) than that in model A (0.5 MPa), indicating the ipsilateral fibula shared load after fusion with talus.
Conclusions: Our computational findings suggest that double-strut fibula ankle arthrodesis is an acceptable construct for distal tibia defect and the ipsilateral fibula shares load after fusion with talus.
Keywords: Bone tumor; Distal tibia; Fibular graft; Finite element analysis.
Conflict of interest statement
Each author certifies that neither he nor any member of his immediate family has funding or commercial associations that might pose a conflict of interest in connection with the submitted article.
Figures

References
-
- Shekkeris AS, Hanna SA, Sewell MD, Spiegelberg BG, Aston WJ, Blunn GW, et al. Endoprosthetic reconstruction of the distal tibia and ankle joint after resection of primary bone tumours. J Bone Joint Surg Br. 2009;91:1378–82. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
