

Expansion of a direct-to-patient telemedicine abortion service in the United States and experience during the COVID-19 pandemic
- PMID: 33781762
- PMCID: PMC9748604
- DOI: 10.1016/j.contraception.2021.03.019
Expansion of a direct-to-patient telemedicine abortion service in the United States and experience during the COVID-19 pandemic
Abstract
Objective: To present updated evidence on the safety, efficacy and acceptability of a direct-to-patient telemedicine abortion service and describe how the service functioned during the COVID-19 pandemic.
Study design: We offered the study at 10 sites that provided the service in 13 states and Washington DC. Interested individuals obtained any needed preabortion tests locally and had a videoconference with a study clinician. Sites sent study packages containing mifepristone and misoprostol by mail and had remote follow-up consultations within one month by telephone (or by online survey, if the participant could not be reached) to evaluate abortion completeness. The analysis was descriptive.
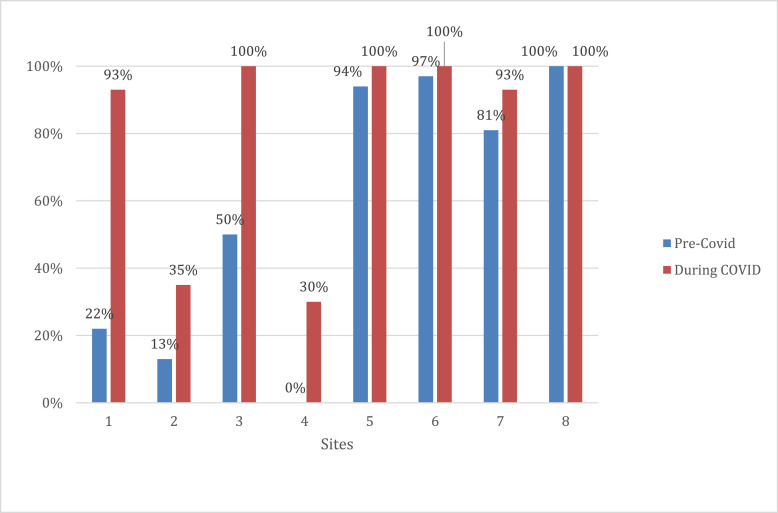
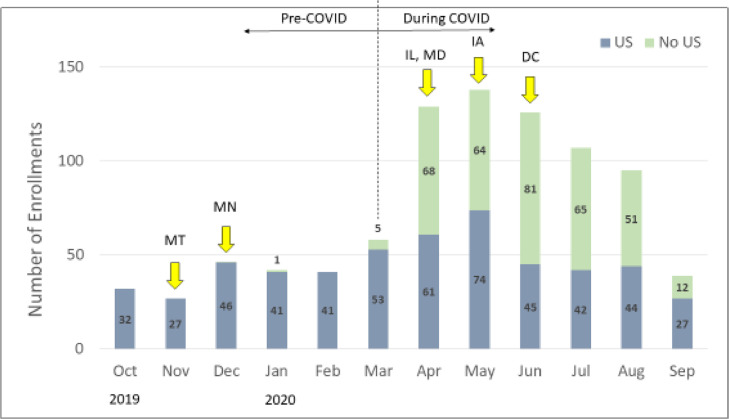
Results: We mailed 1390 packages between May 2016 and September 2020. Of the 83% (1157/1390) of abortions for which we obtained outcome information, 95% (1103/1157) were completed without a procedure. Participants made 70 unplanned visits to emergency rooms or urgent care centers for reasons related to the abortion (6%), and 10 serious adverse events occurred, including 5 transfusions (0.4%). Enrollment increased substantially with the onset of COVID-19. Although a screening ultrasound was required, sites determined in 52% (346/669) of abortions that occurred during COVID that those participants should not get the test to protect their health. Use of urine pregnancy test to confirm abortion completion increased from 67% (144/214) in the 6 months prior to COVID to 90% (602/669) in the 6 months during COVID. Nearly all satisfaction questionnaires (99%, 1013/1022) recorded that participants were satisfied with the service.
Conclusions: This direct-to-patient telemedicine service was safe, effective, and acceptable, and supports the claim that there is no medical reason for mifepristone to be dispensed in clinics as required by the Food and Drug Administration. In some cases, participants did not need to visit any facilities to obtain the service, which was critical to protecting patient safety during the COVID-19 pandemic.
Implications: Medical abortion using telemedicine and mail is effective and can be safely provided without a pretreatment ultrasound. This method of service delivery has the potential to greatly improve access to abortion care in the United States.
Keywords: COVID-19; Mail; Medical abortion; Telemedicine; United States.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures
References
-
- Kohn JE, Snow JL, Simons HR, Seymour JW, Thompson TA, Grossman D. Medication abortion provided through telemedicine in four U.S. states. Obstet Gynecol. 2019;134(2):343–350. - PubMed
-
- Fix L, Seymour JW, Sandhu MV, Melville C, Mazza D, Thompson TA. At-home telemedicine for medical abortion in Australia: a qualitative study of patient experiences and recommendations. BMJ Sex Reprod Health. 2020;46:172–176. - PubMed
-
- Ehrenreich K, Kaller S, Raifman S, Grossman D. Women's experiences using telemedicine to attend abortion information visits in Utah: A qualitative study. Women's. Health Issues. 2019;29(5):407–413. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
