

Heart Failure Hospitalization Risk associated with Iron Status in Veterans with CKD
- PMID: 33782035
- PMCID: PMC8092060
- DOI: 10.2215/CJN.15360920
Heart Failure Hospitalization Risk associated with Iron Status in Veterans with CKD
Abstract
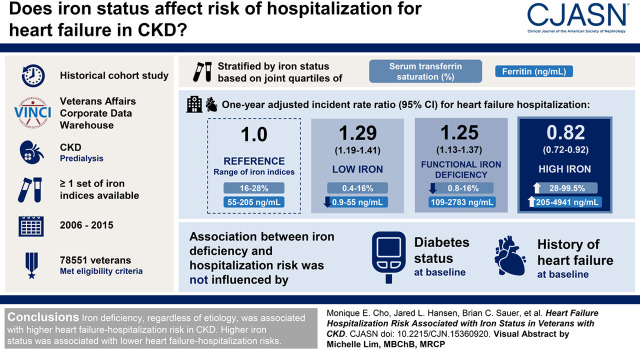
Background and objectives: CKD is an independent risk factor for heart failure. Iron dysmetabolism potentially contributes to heart failure, but this relationship has not been well characterized in CKD.
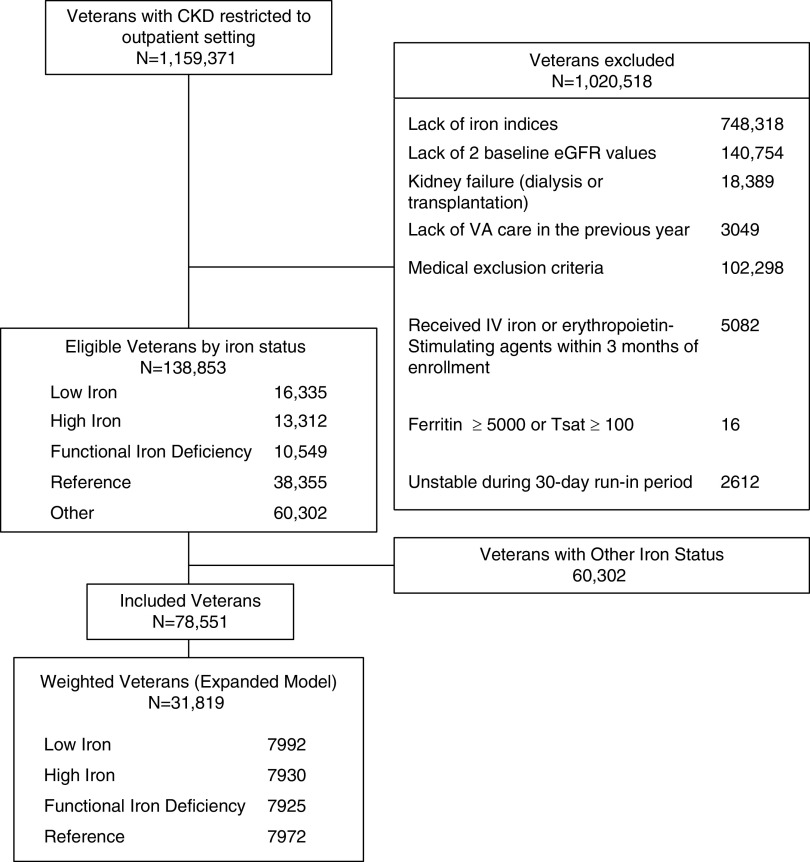
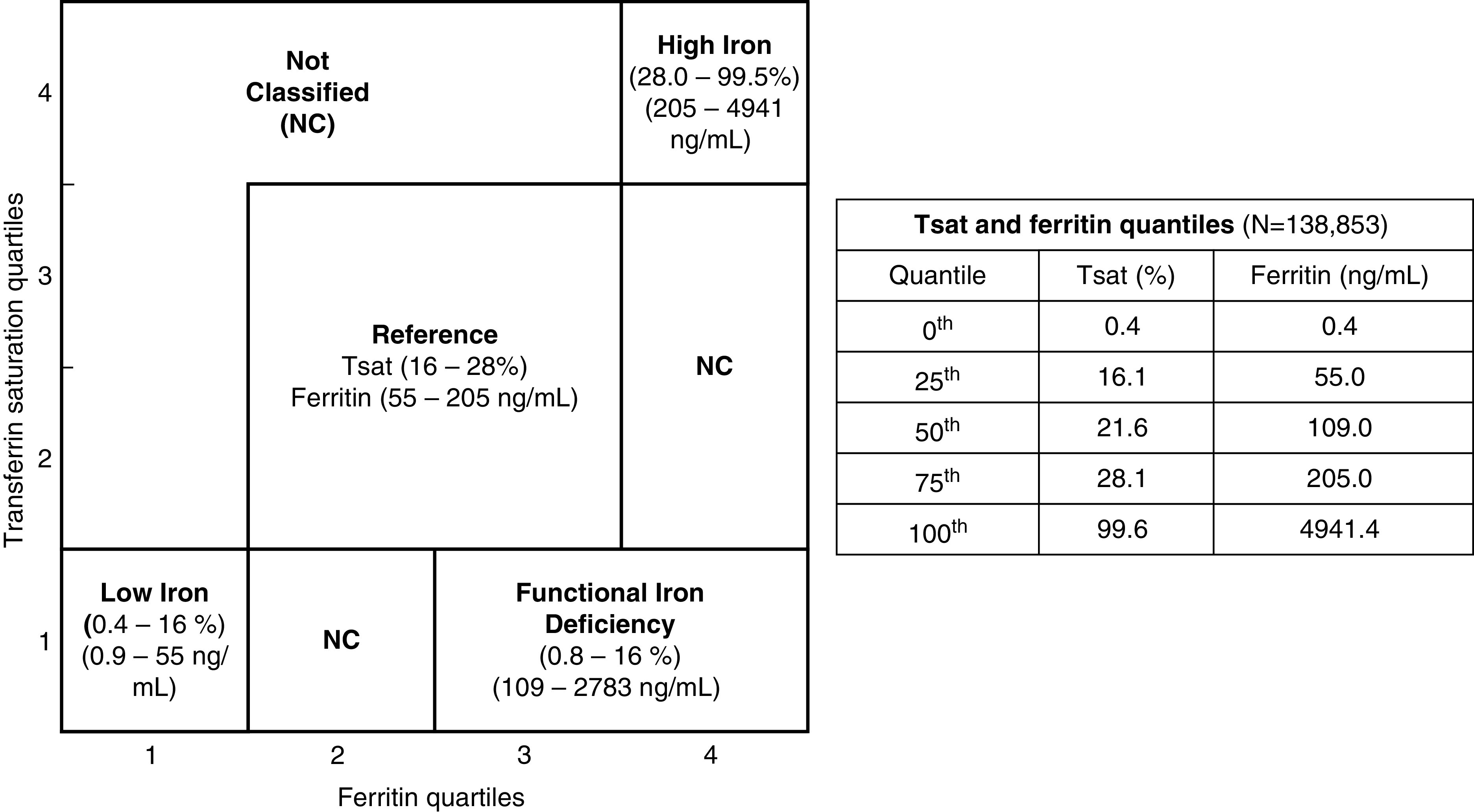
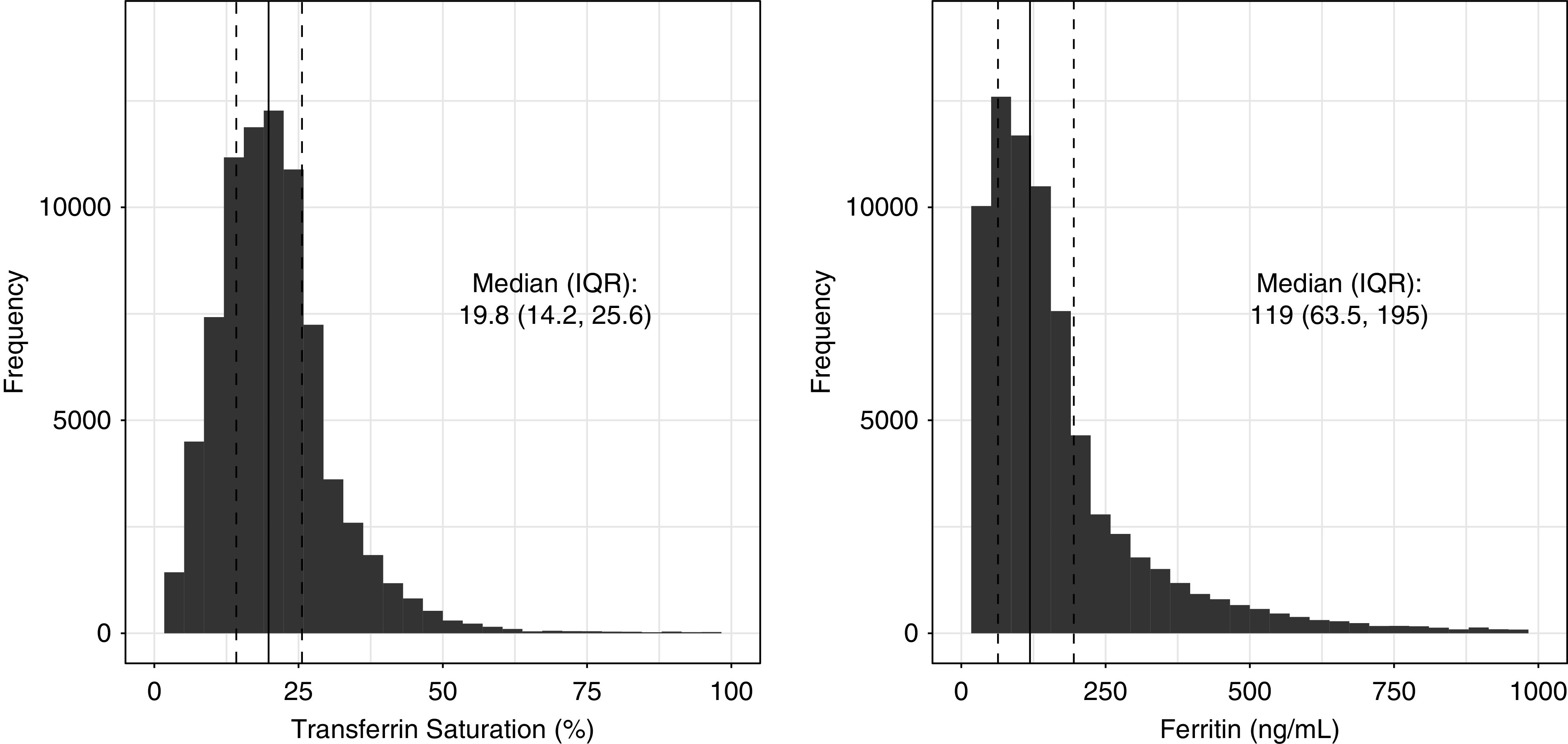
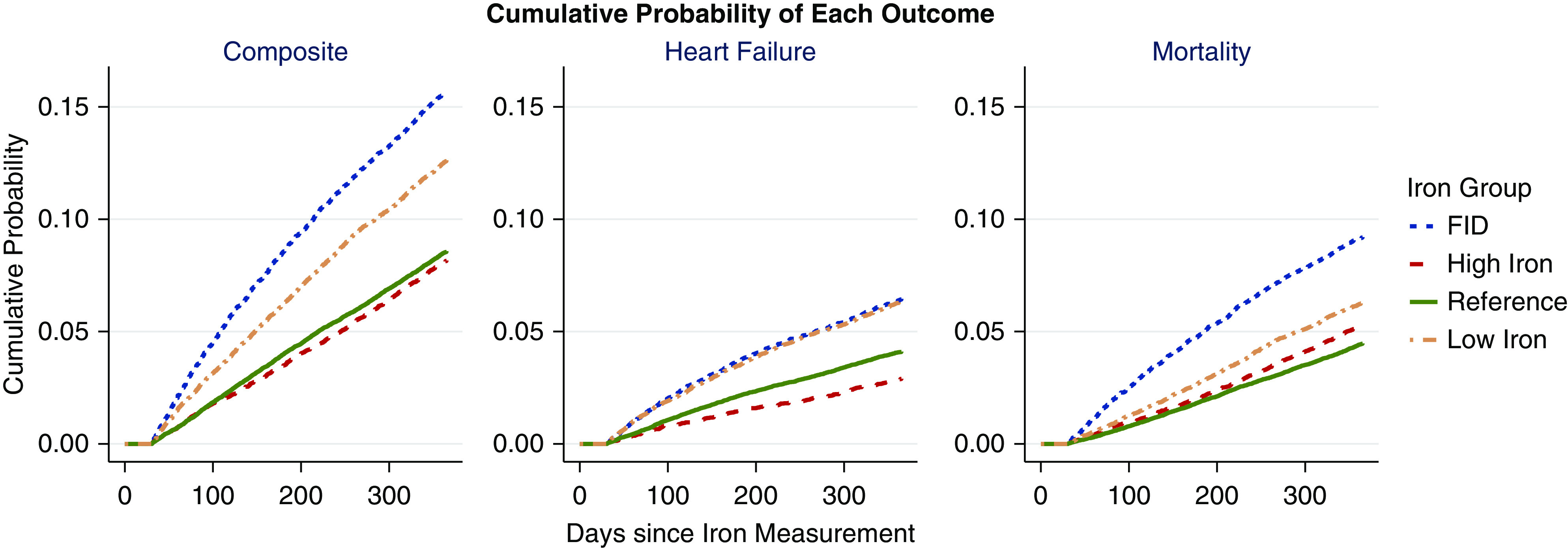
Design, setting, participants, & measurements: We performed a historical cohort study using data from the Veterans Affairs Corporate Data Warehouse to evaluate the relationship between iron status and heart failure hospitalization. We identified a CKD cohort with at least one set of iron indices between 2006 and 2015. The first available date of serum iron indices was identified as the study index date. The cohort was divided into four iron groups on the basis of the joint quartiles of serum transferrin saturation (shown in percent) and ferritin (shown in nanograms per milliliter): reference (16%-28%, 55-205 ng/ml), low iron (0.4%-16%, 0.9-55 ng/ml), high iron (28%-99.5%, 205-4941 ng/ml), and function iron deficiency (0.8%-16%, 109-2783 ng/ml). We compared 1-year heart failure hospitalization risk between the iron groups using matching weights derived from multinomial propensity score models and Poisson rate-based regression.
Results: A total of 78,551 veterans met the eligibility criteria. The covariates were well balanced among the iron groups after applying the propensity score weights (n=31,819). One-year adjusted relative rate for heart failure hospitalization in the iron deficiency groups were higher compared with the reference group (low iron: 1.29 [95% confidence interval, 1.19 to 1.41]; functional iron deficiency: 1.25 [95% confidence interval, 1.13 to 1.37]). The high-iron group was associated with lower 1-year relative rate of heart failure hospitalization (0.82; 95% confidence interval, 0.72 to 0.92). Furthermore, the association between iron deficiency and heart failure hospitalization risk remained consistent regardless of the diabetes status or heart failure history at baseline.
Conclusions: Iron deficiency, regardless of cause, was associated with higher heart failure hospitalization risk in CKD. Higher iron status was associated with lower heart failure hospitalization risks.
Keywords: CKD; chronic kidney disease; heart failure; hospitalization; iron; veterans.
Copyright © 2021 by the American Society of Nephrology.
Figures
Comment in
-
A New View of Iron Management in Heart Failure: What Nephrologists Need to Know.Clin J Am Soc Nephrol. 2021 Apr 7;16(4):502-504. doi: 10.2215/CJN.01850221. Epub 2021 Mar 29. Clin J Am Soc Nephrol. 2021. PMID: 33782037 Free PMC article. No abstract available.
References
-
- Kottgen A, Russell SD, Loehr LR, Crainiceanu CM, Rosamond WD, Chang PP, Chambless LE, Coresh J: Reduced kidney function as a risk factor for incident heart failure: The Atherosclerosis Risk in Communities (ARIC) study. J Am Soc Nephrol 18: 1307–1315, 2007 - PubMed
-
- Anand IS, Gupta P: Anemia and iron deficiency in heart failure: Current concepts and emerging therapies. Circulation 138: 80–98, 2018 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
