

Burden of noninfluenza respiratory viral infections in adults admitted to hospital: analysis of a multiyear Canadian surveillance cohort from 2 centres
- PMID: 33782171
- PMCID: PMC8099164
- DOI: 10.1503/cmaj.201748
Burden of noninfluenza respiratory viral infections in adults admitted to hospital: analysis of a multiyear Canadian surveillance cohort from 2 centres
Abstract
Background: Data on the outcomes of noninfluenza respiratory virus (NIRV) infections among hospitalized adults are lacking. We aimed to study the burden, severity and outcomes of NIRV infections in this population.
Methods: We analyzed pooled patient data from 2 hospital-based respiratory virus surveillance cohorts in 2 regions of Canada during 3 consecutive seasons (2015/16, 2016/17, 2017/18; n = 2119). We included patients aged ≥ 18 years who developed influenza-like illness or pneumonia and were hospitalized for management. We included patients confirmed positive for ≥ 1 virus by multiplex polymerase chain reaction assays (respiratory syncytial virus [RSV], human rhinovirus/enterovirus (hRV), human coronavirus (hCoV), metapneumovirus, parainfluenza virus, adenovirus, influenza viruses). We compared patient characteristics, clinical severity conventional outcomes (e.g., hospital length-of stay, 30-day mortality) and ordinal outcomes (5 levels: discharged, receiving convalescent care, acute ward or intensive care unit [ICU] care and death) for patients with NIRV infections and those with influenza.
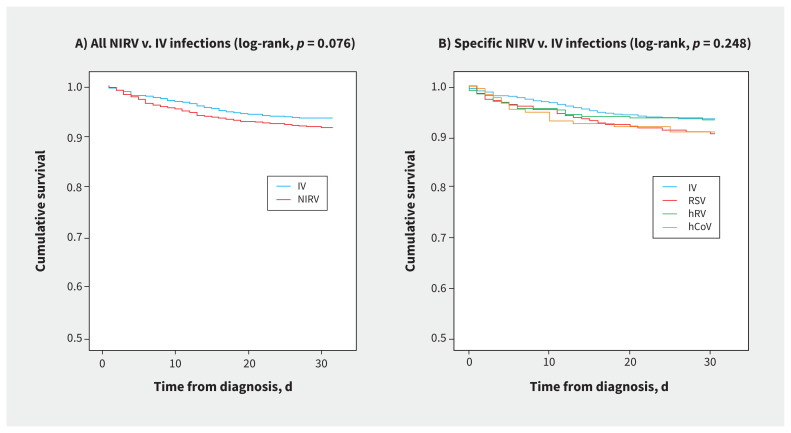
Results: Among 2119 adults who were admitted to hospital, 1156 patients (54.6%) had NIRV infections (hRV 14.9%, RSV 12.9%, hCoV 8.2%) and 963 patients (45.4%) had influenza (n = 963). Patients with NIRVs were younger (mean 66.4 [standard deviation 20.4] yr), and more commonly had immunocompromising conditions (30.3%) and delay in diagnosis (median 4.0 [interquartile range (IQR) 2.0-7.0] days). Overall, 14.6% (12.4%-19.5%) of NIRV infections were acquired in hospital. Admission to ICU (18.2%, median 6.0 [IQR 3.0-13.0] d), hospital length-of-stay (median 5.0 [IQR 2.0-10.0] d) and 30-day mortality (8.4%; RSV 9.5%, hRV 6.6%, hCoV 9.2%) and the ordinal outcomes were similar for patients with NIRV infection and those with influenza. Age > 60 years, immunocompromised state and hospital-acquired viral infection were associated with worse outcomes. The estimated median cost per acute care admission was $6000 (IQR $2000-$16 000).
Interpretation: The burden of NIRV infection is substantial in adults admitted to hospital and associated outcomes may be as severe as for influenza, suggesting a need to prioritize therapeutics and vaccines for at-risk people.
© 2021 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: Nelson Lee declares honoraria for consultancy work, speaking in educational programs or travel support from Shionogi, Gilead Sciences Canada, Janssen Pharmaceuticals, Sanofi-Pasteur, F. Hoffmann-La Roche, Genentech, CIDARA Therapeutics, outside the submitted work. Scott Klarenbach is supported by the Kidney Health Research Chair, and the Division of Nephrology at the University of Alberta, outside the submitted work.
Figures


References
-
- GBD 2016 Lower Respiratory Infections Collaborators; Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis 2018;18:1191–210. - PMC - PubMed
-
- Zhou F, Wang Y, Liu Y, et al. .; CAP-China Network. Disease severity and clinical outcomes of community-acquired pneumonia caused by non-influenza respiratory viruses in adults: a multicentre prospective registry study from the CAP-China Network. Eur Respir J 2019;54:1802406. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical